Article Text

Statistics from Altmetric.com
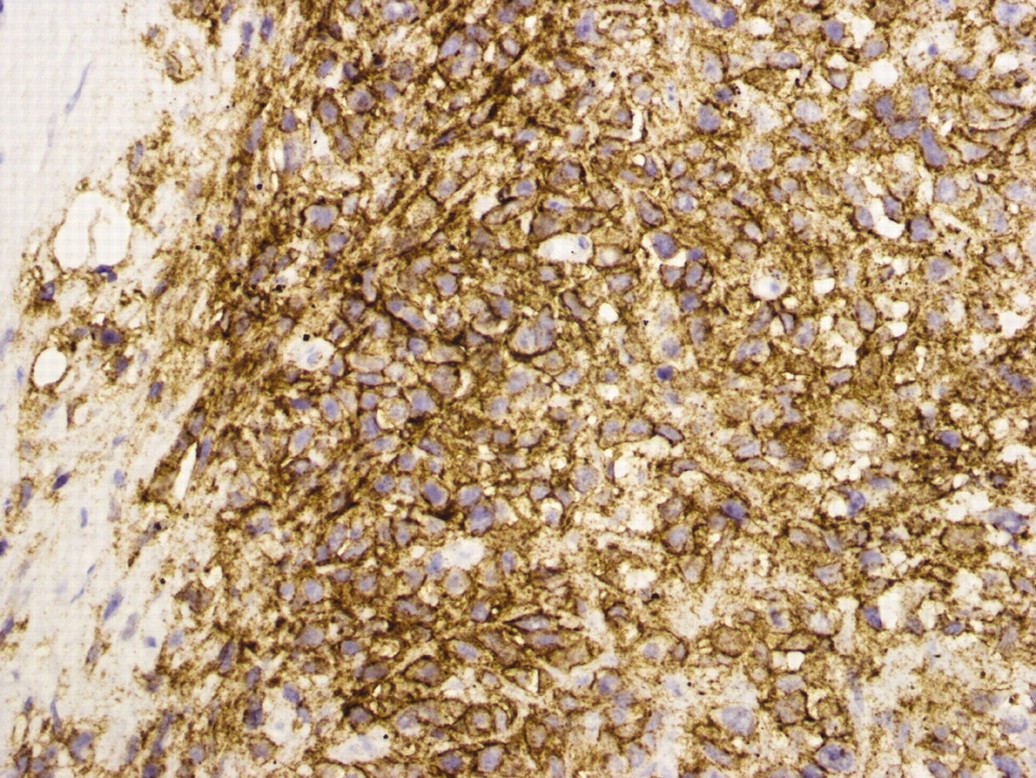
A 65-year-old man, previously well, presented with a 2 week history of abdominal pain and fever. Splenomegaly and jaundice were present, with no peripheral lymphadenopathy and no clinical evidence of bacterial endocarditis. Blood tests showed mild anaemia (haemoglobin 10 g/dl), pronounced thrombocytopenia, bilirubin 102 µmol/l (66 conjugated), and a positive Coombs test. Computed tomography (CT) scan of the abdomen (fig 1) showed splenomegaly with areas of altered perfusion suggestive of infarction, and no other abnormality. Bone marrow aspirate was normal and blood cultures were negative. He developed progressive renal and hepatic failure and died within 6 days of presentation of multiple organ failure with severe lactic acidosis. Postmortem examination showed a highly aggressive B cell lymphoma (fig 2) confined to the liver and spleen with areas of necrosis. All tumour cells are CD20 positive indicating B cell phenotype. Bone sections done postmortem also confirmed the diagnosis.

Computed tomography image showing splenomegaly with splenic infarctions (arrow).

{kind=link}
{kind=link}
Splenic lymphoma showing all tumour cells positive for CD20 immunoperoxidase (Brown staining is positive).
Causes for splenic infarction1–3 include thromboembolic disorders, haematologic disease (haemoglobinopathies, leukaemia, lymphoma, myelofibrosis, polycythemia vera), splenic vascular disease, vasculitis, portal hypertension, infiltrative disorders, and pancreatic disease.
The areas of altered splenic perfusion on CT scan were not due to embolic infarction but to necrosis caused by the tumour outgrowing its blood supply. Splenic lymphomas are usually low grade, allowing adequate time to perform diagnostic splenectomy. Absence of peripheral lymphadenopathy and rapid clinical progression with necrosis made this case an unusual presentation. There is also a possibility that an earlier diagnosis could have been made if trephine had been done along with bone marrow aspiration.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication