Article Text

Statistics from Altmetric.com
An 83-year-old man presented to the emergency department with haematemesis and collapse for 1 day. He was fit and well before admission with no significant past medical history. After transfusing 4 units of blood, the patient was stabilised and the haematemesis stopped spontaneously. He gave a history of epigastric pain for 3 days but no maelena, dysphagia or weight loss. Subsequent urgent oesophago-gastrodudenoscopy revealed blood clot and food debris inside the oesophagus. There was a clear mass arising from the oesophageal wall which was suspected to be tumour (fig 1). Chest x-ray showed a left hilar shadow (fig 2). Based on a suspicion of oesophageal tumour, an urgent computed tomography (CT) scan was done (fig 3). The CT scan showed a thoraco-abdominal dissecting aneurysm with no evidence of leak or fistula between the aorta and the oesophagus. The oesophagus was filled with food debris and blood clot, but there was no oesophageal mass or tumour.
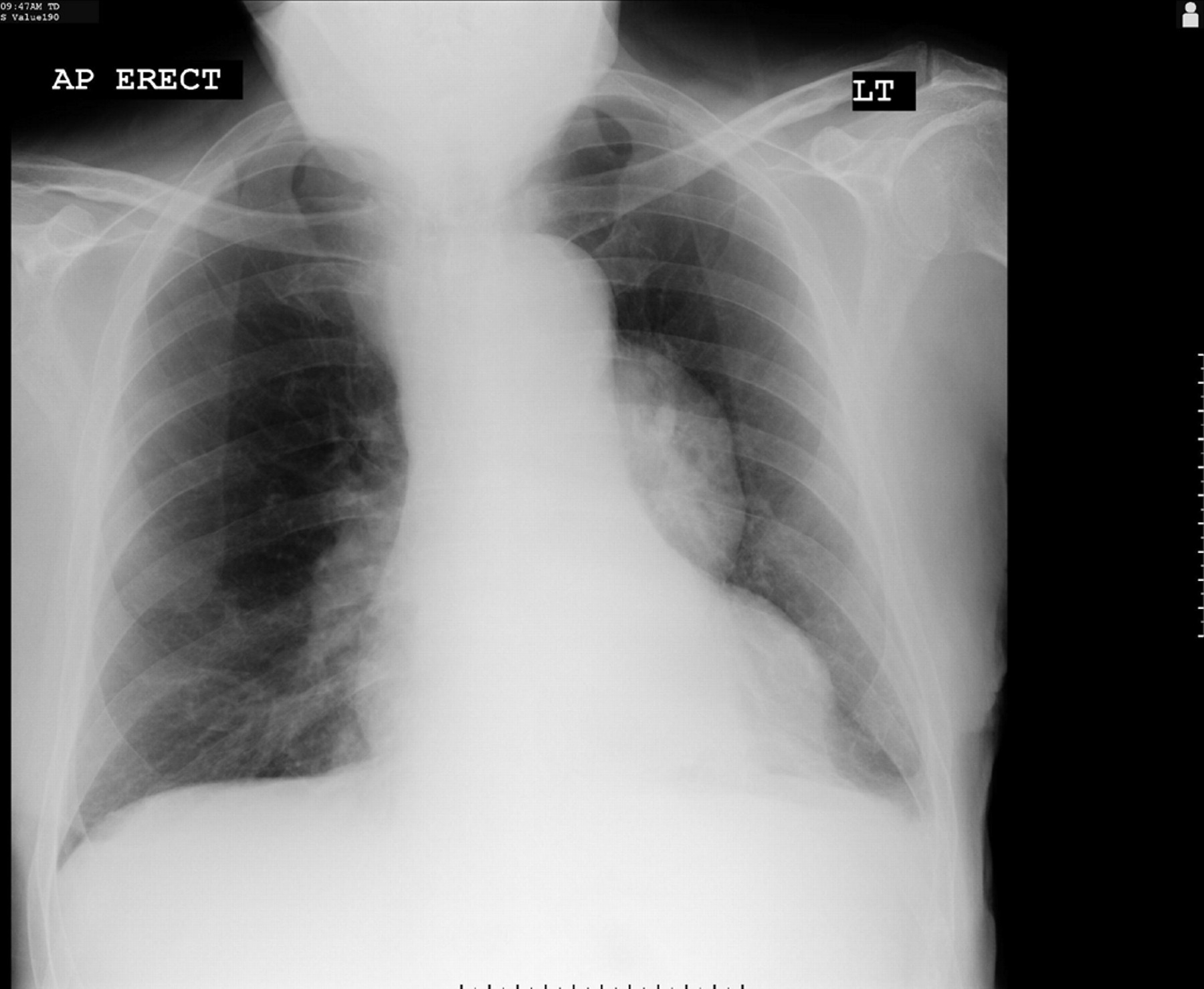
Chest x-ray showing a left hilar shadow.

An endoscopic image of the oesophageal lumen filled with debris and blood clot.

{kind=link}
{kind=link}
{kind=link}
Computed tomography scan showing a dissecting aortic aneurysm.
The man was stabilised and an urgent referral was done to a tertiary centre. Unfortunately, shortly afterward, the patient suddenly had a cardiac arrest and haematemesis which became out of control, and he died. Post mortem examination found a ruptured thoracic aortic aneurysm as the cause of death.
Learning points
-
Dissecting aneurysm may present with heamatemesis due to aorto-oesophageal leak or fistula.1
-
Aortic dissection is an uncommon but a potentially fatal condition. A high level of suspicion is required for successful diagnosis and management.2
-
Rapid intervention is required because delay leads to higher mortality.
-
Despite advances in diagnostic and therapeutic techniques, mortality and morbidity of dissecting aortic aneurysm is still high.3
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication