Article Text

Summary
We report the case of a 9-year-old child with asthma, atopic dermatitis and allergic rhinoconjunctivitis due to house dust mites, in whom a routine chest x-ray identified by chance abnormal organ position, such as the stomach located on the right side. Abdominal ultrasonography indicated a centralised liver, with polysplenia on the right side and an inferior cava vein located to the left of the aorta with no interruption. Ultrasonography did not show heart defects. Magnetic resonance imaging (MRI) of the abdomen was performed that showed a short pancreas, with no neck, body and tail in it, and a left inferior vena cava with normal outlet of the renal veins, and absence of the intrahepatic part of the inferior vena cava, that was replaced by the left hemiazygos vein. Spinal cord MRI revealed dorsal syringomelia. In view of the results obtained, the diagnosis of situs ambiguous was established.
Statistics from Altmetric.com
Background
Situs solitus is defined as the normal position of organs. Situs ambiguous is a rare congenital defect where most organs are heterogeneously distributed in the chest and abdomen. In addition to the left/right axis inversion with partial or complete situs inversus, laterality can be left (left isomerism) or right (right isomerism). Isomerism is defined as a defect in the asymmetry of paired organs.1 The left–right axis is defined in the early stages of embryogenesis,2–5 approximately around day 15. Isomerisms can be isolated, but can also be part of various syndromes, the best known of which—for its respiratory disorders—is immotile cilia, that includes Kartagener syndrome. This syndrome shows a recessive inheritance and is associated with situs inversus, heart defects, bronchiectasis, sinusitis, and otitis media as well as sterility in males. The main disorder includes structural anomalies of the cilia of the respiratory mucosa.6
Abnormal intestinal rotations are commonly found in patients with heterotaxy syndrome.1,7 The pancreas, duodenum, stomach, liver and spleen are involved in some form of rotation in the early stages of embryonic development, generally between weeks 5 and 6 of pregnancy.8 It is likely that the effect of a nosological factor during this period can cause incomplete or reverse rotation in some organs. Therefore, heterotaxy can also cause polysplenia or asplenia associated with congenital heart defects. The heterotaxy syndrome associated with asplenia has a worse prognosis, because it is commonly associated with significant heart anomalies.9,10 However, the advances made in recent years in heart surgery and the early detection of heart disorders by prenatal ultrasonography have prolonged survival in patients with heterotaxy.7,11 It has also been shown that some maternal diseases, such as diabetes mellitus, increase the risk of cardiac malformations and heterotaxy in newborns.12 Situs ambiguous can be considered as a symptom complex rather than a diagnosis. The pathophysiology of syringomyelia changes with different types. In the cases associated with the malformation of the cranium cervical, the cerebrospinal fluid cannot flow freely from the ventricle IV towards the subarachnoid space. The most common reason is the decrease of the cerebellar tonsils below the foramen magnum in the Chiari.
We report the case of a child who, when undergoing a diagnostic procedure for allergic disease (bronchial asthma), was by chance diagnosed with situs ambiguous.
Case presentation
A 9-year-old child who had experienced episodes of bronchospasms since the age of 1 year was presented. These episodes were associated with atopic dermatitis, recurrent hives, and seasonal rhinoconjunctivitis. The child’s mother had a normal pregnancy and perinatal period, although the mother and maternal grandfather both had a history of allergic rhinoconjunctivitis. The child’s was being treated with montelukast 5 mg, one tablet daily.
Investigations
The physical examination showed positive dermographism, but all other findings were normal. The following additional examinations were performed. Complete blood count: eosinophils 2.7%, IgE 156 kU/l. Prick test: Dermatophagoides pteronyssimus (dp) and farinae (df), CAP to dp: 32.90 kU/l, and df: 24 kU/l; Ig G, Ig A and Ig M normal. Cavum x-ray: adenoid hypertrophy. Basal spirometry and bronchodilation test: negative. X-ray of paranasal sinus: normal. The chest x-ray showed no significant disorders in the lungs, the right side of the stomach, and prominent azygos vein (fig 1), so it was decided to perform an abdominal ultrasonography.

Chest x-ray showing the right side of the stomach and the prominence of the azygos vein.
Outcome and follow-up
Abdominal ultrasonography showed: a centralised liver, though mainly on the left side, with the bladder on the right side; polysplenia on the right side; normal kidneys; the inferior vena cava on the left side of the aorta with no interruption; no splenic vein or pancreas; and levocardia (fig 2).

Ultrasonographic evidence of polysplenia. Panels A and B show two independent spleens.
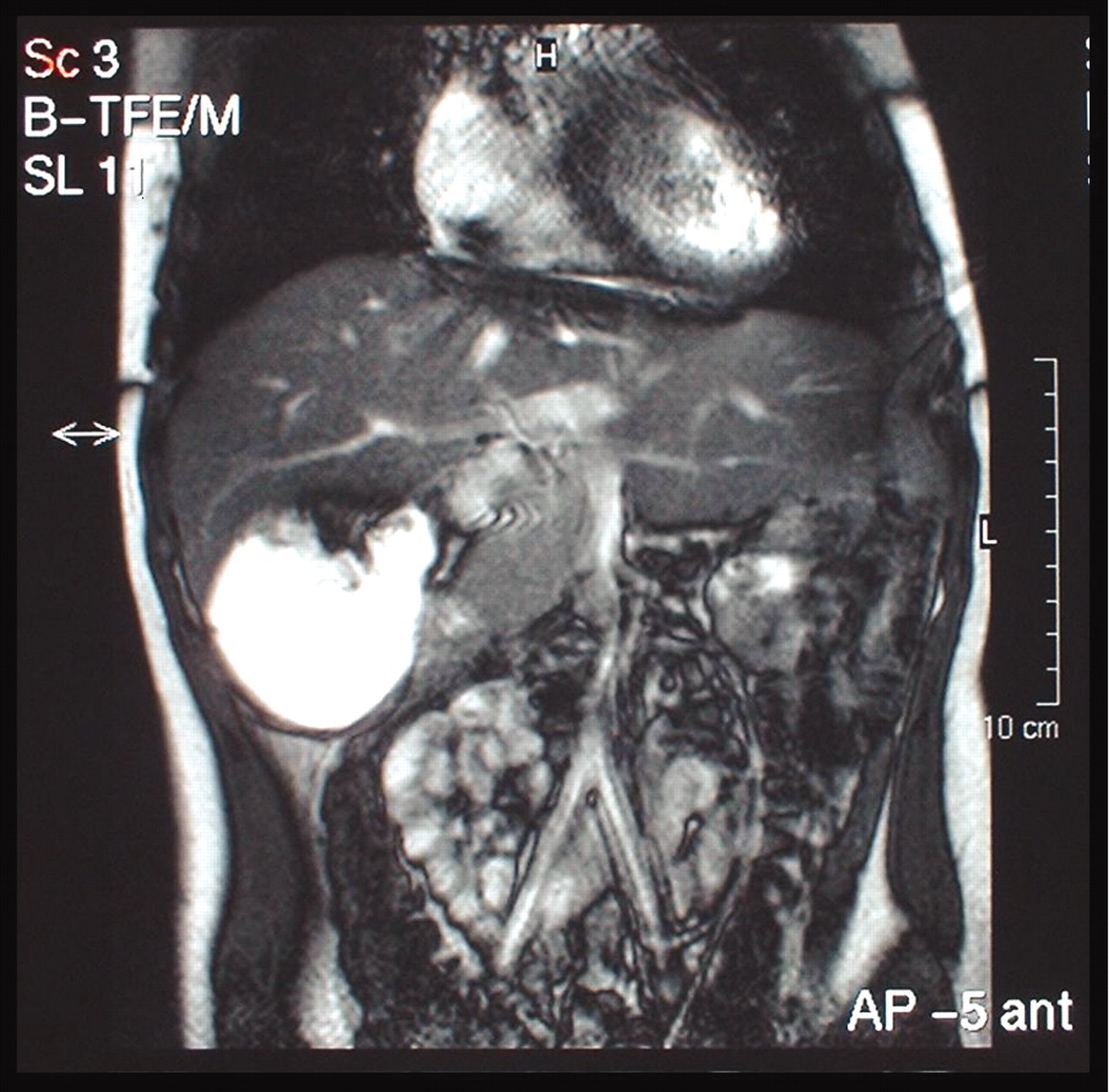
Ultrasonography showed: situs auricular solitus; normal atrioventricular and arterial–ventricular connections; integer intracardial walls; no significant valvular diseases; normal global and segmentary ventricular function; no ductus or aortic coarctation. Abdominal magnetic resonance imaging (MRI) showed: short pancreas, with a larger sized head and no neck, body and tail; left inferior vena cava with normal outlet of renal veins; no intrahepatic part of the lower cava vein, which was replaced by left hemiazygos vein to the thoraco-abdominal junction where drainage continued with the right azygos vein; and low dorsal syringomyelia (fig 3). Spinal cord and posterior fossa MRI showed: prominence of the ependimary duct in the marrow cone, with anomalies in the roots of the horsetail; no lesions in the posterior fossa (fig 4).
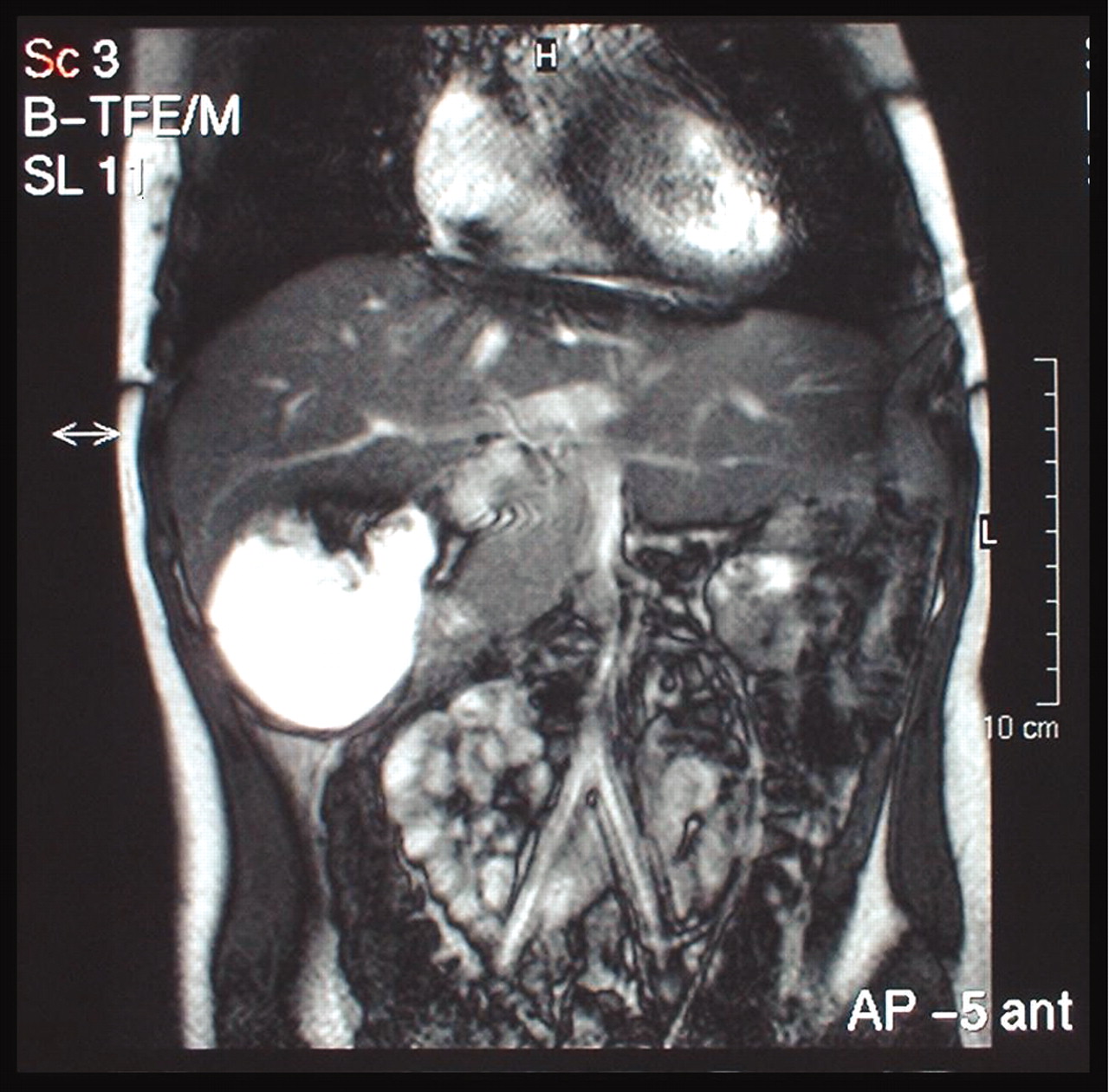
Abdominal magnetic resonance image showing absence of the intrahepatic part of the lower cava vein, that has been replaced by the left hemiazygos vein. The centralised heart and an enlarged liver are also shown.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Spinal cord MRI, showing the area with hydrosyringomyelia.
In view of all the above findings, a diagnosis of situs ambiguous was made.
Discussion
The best way to classify and diagnose abnormal heart positions is by segmentary approaches, first identifying the position of the organs and the atria, then the ventricles, and finally the large vessels. The determination of visceroatrial situs can be made by radiographic determination of the position of the abdominal organs and tracheal bifurcation, to recognise the left and right bronchi, and by ultrasonography. The atria situs is related to visceral and pulmonary situs. In situs solitus, the organs are in their normal position (stomach and spleen to the left, liver to the right); the right tri-lobed lung is located on the right and the left bi-lobed on the left; and the right atrium is located on the right, while the left atrium is located on the left. When the abdominal organs and the lungs are inverted—a condition known as situs inversus—the left atrium is located on the right and the right atrium on the left. If the visceroatrial situs cannot be easily established, this is a condition called undetermined situs or heterotaxy.9,13,14 The main two varieties are: (1) asplenia syndrome (right isomerism or bilateral right aspect), and is associated with a liver located in the central position, lack of spleen, and two morphologically right lungs; and (2) polysplenia syndrome15 (left isomerism or bilateral left aspect), which is associated with multiple spleens which are small in size, absence of the intrahepatic area of the inferior vena cava, and left morphology of both lungs.6,16 The heterotaxy syndromes are usually associated with severe congenital heart diseases: interauricular communication (IAC), interventricular communication (IVC), atrioventricular communication, pulmonary stenosis or atresia, and abnormal pulmonary systemic venous return.16,17 In the presence of situs solitus, the right atrium is connected to the left ventricle and the left atrium is connected to the right ventricle (ventricular inversion).
The final segment is of the large vessels. With each type of cardiac loop, the ventriculoarterial ratios can be considered as normal (right ventricle to the pulmonary artery and left ventricle to the aorta) or transposed (right ventricle to the aorta and left ventricle to the pulmonary aorta). An additional classification can be made, based on the position of the aorta (usually located in the right and behind), related to the pulmonary artery. In the transposition, the aorta is usually located front and on the right of the pulmonary artery (d-transposition) or on the left (l-transposition). These segmentary ratios can be measured by echocardiographic and angiographic examinations.13,18 The clinical manifestations of these syndromes of heart malposition are determined particularly by the cardiovascular malformations associated with them.
Dextrocardia occurs when the heart is located on the right side of the chest, and levocardia (normal position) exists when the heart is located on the left side of the chest. Dextrocardia with no associated situs inversus and levocardia in the presence of situs inversus are almost always associated with severe malformations. Studies performed in older children and adults show that dextrocardia with situs inversus and large vessels with normal ratios (the so-called dextrocardia with specular image) is often associated with functionally normal hearts, though less severe congenital heart diseases are also common.
Anatomic or functional anomalies of the lungs, diaphragm and chest box can cause displacement of the heart to the right (dextroposition). However, the heart vortex usually still points to the left. This anatomic position is less frequently associated with congenital heart disease, though hypoplasia of one lung can be associated with abnormal pulmonary venous return of that lung (scimitar syndrome).
The electrocardiogram is difficult to interpret in the presence of heart disease with disagreement of atrial, ventricular and large vessel anatomy. The diagnosis usually requires a detailed study by echocardiography and cardiac catheterisation. The prognosis and treatment of patients with cardiac malposition are determined by underlying heart diseases. Asplenia increases the risk of severe infections such as bacterial sepsis, which makes daily antibiotic prophylaxis necessary. The risk of sudden death due to arrhythmia occurring after palliative surgery is also increased.
The following can be concluded: (1) in this case, a routine chest x-ray identified the associated malformations; (2) given the left isomerism with polysplenia and the male sex, it is advisable to test ciliary motility and fertility in old age to rule out Kartagener syndrome.11
Learning points
-
Situs ambiguous is a rare congenital defect where most organs are heterogeneously distributed in the chest and abdomen.
-
The heterotaxy syndromes are usually associated with severe congenital heart diseases.
-
Routine chest x-ray can identify associated malformations.
REFERENCES
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication