Article Text

Statistics from Altmetric.com
A 3-day-old, full-term male neonate born by a caearean section for obstructed labour presented with respiratory distress beginning within hours of birth. There was no history of prolonged rupture of membranes or maternal fever.
The baby cried immediately after birth and there was no need for resuscitation.
Antenatal sonography done at the referring centre had detected some abnormality in the posterior cranial fossa, described as “Dilated foramen magnum” (images not available).
The baby weighed 3.5 kg and had an OFC (occipitofrontal circumference) of 36.5 cm.
The anterior and posterior fontanel were wide open, the sutures were widely separate and the occiput was very prominent (fig 1) The respiratory rate was 118/min; respiration was jerky and irregular, followed by apnoea. The respiratory distress may have been because of transient tachypnoea.

Large head with occipital prominence.
Other systemic examinations were normal.
Transillumination of the skull was negative and there was no cranial bruit.
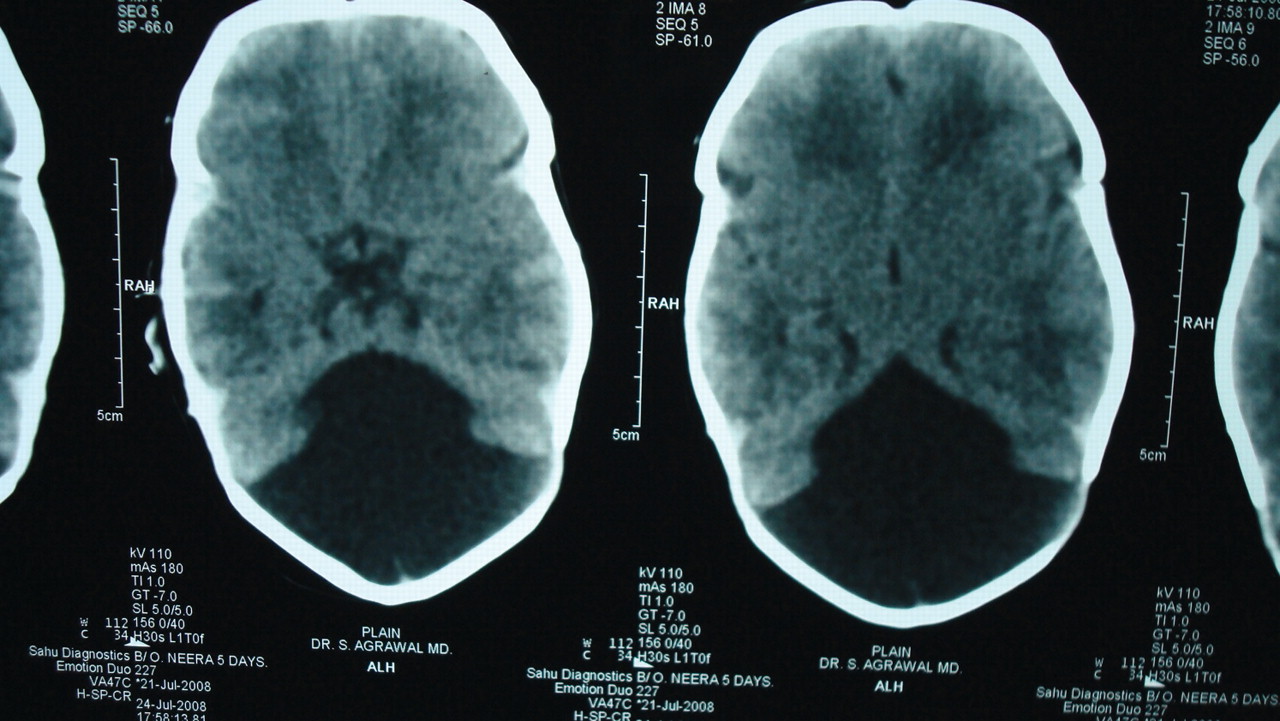
A CT scan of the head showed a dilated fourth ventricle and hypoplastic cerebellar hemispheres with splaying and agenesis of the corpus callosum. There was no hydrocephalus. (figs 2 and 3)

Dilated fourth ventricle.
{kind=link}
{kind=link}
{kind=link}
Hypoplastic cerebellar vermis.
A diagnosis of Dandy–Walker malformation was made.
The classical Dandy–Walker malformation is characterised by cystic dilatation of the fourth ventricle, which almost fills the entire enlarged posterior fossa; the cerebellar vermis is hypoplastic and rotated or aplastic, and the tentorium and torcula are elevated.1
Approximately 90% of patients have hydrocephalus, and a significant number of children have associated anomalies, including agenesis of the posterior cerebellar vermis and corpus callosum.
The Dandy–Walker malformation is managed by shunting the cystic cavity (and on occasion the ventricles as well) in the presence of hydrocephalus.2
This baby does not have hydrocephalus currently (but is likely to develop it postnatally), hence no shunting was considered.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.