Article Text

Statistics from Altmetric.com
DESCRIPTION
A 58-year-old man was admitted with a 2 week history of worsening, painful, itchy lesions on his right upper chest, axilla and upper back. A year before, he had been treated for chronic myeloid leukaemia with chemotherapy and was under remission on maintenance corticosteroid therapy.
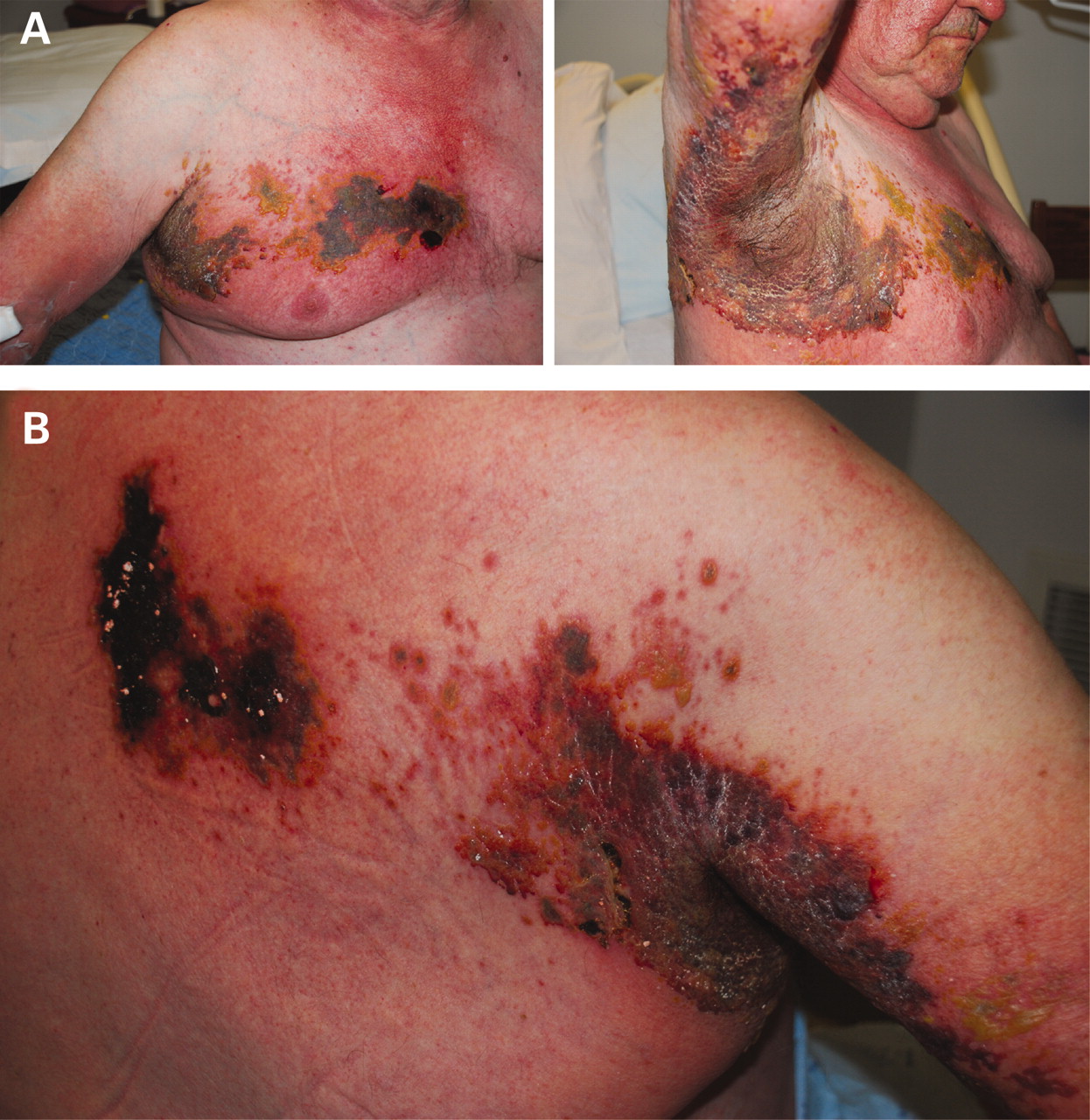
Examination revealed a rash involving dermatomes T1 and T2 9 (fig 1A) with multiple grouped vesicles, a few pustules and extensive blackish, adherent crusts with underlying erosions (fig 1B). Laboratory tests revealed neutrophilic leucocytosis. Clinical diagnosis was consistent with erosive herpes zoster. Intravenous acyclovir was initiated for a total of 5 days with good clinical response. He was discharged home to continue oral aciclovir with a follow-up in 1 week.

{kind=link}
(A) Severe herpes zoster involving dermatomes T1 and T2. (B) Multiple grouped vesicles, a few pustules and extensive blackish adherent crusts with underlying erosions noted.
Herpes zoster infection is more common in immunosuppressed patients and tends to be severe with multiple dermatomal involvement and visceral dissemination. Potential life threatening complications like hepatitis, pneumonia or encephalitis have also been described. Diagnosis is usually on clinical grounds, with the appearance of a characteristic rash in a dermatomal distribution. Early institution of therapy with intravenous acyclovir or oral valacyclovir is the cornerstone of therapy.1
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.