Article Text

Statistics from Altmetric.com
Urgent haemodialysis was started in a 66-year-old woman with uraemic drowsiness and a history of chronic kidney disease (CKD) (stage 5, blood urea nitrogen (BUN) 141.3 mg/dl, creatinine 14.8 mg/dl) with poorly controlled hypertension (baseline level 190/75 mm Hg). Her consciousness cleared 3 days later. After a 1 week course of conventional 4 h haemodialysis, she suddenly experienced generalised tonic seizures with bilateral pupil dilatation and a deep coma (Glasgow Coma Scale (GCS) E1M1V1) ensued. The blood pressure peak on that day was 162/89 mm Hg and heart rate was 85 beats/min. Brain magnetic resonance imaging (MRI) study disclosed extensive hyperintensity on T2 weighted images in the white matter of the cerebrum bilaterally (fig 1A) and a severe mass effect with transtentorial herniation compressing the brainstem (fig 1C). After her blood pressure was controlled to 120/80 mm Hg and increased intracranial pressure (ICP) was treated by mannitol infusion with concomitant continuous venovenous haemofiltration, the seizures stopped and her consciousness level improved to E3M5V3 1 week later. In serial follow-up MRIs of the brain at 7 day (fig 2) and 50 day intervals (fig 3), all previous lesions disappeared after her drowsiness was fully alleviated (GCS E4M6V5). Posterior reversible encephalopathy syndrome (PRES) was diagnosed by the typical presentation and MRI patterns.

T2 weighted magnetic resonance images of the brain on day 1 (from left to right, at the level of centrum semiovale, thalamus, and midbrain in order; this order applied to all figures) revealed diffuse symmetric confluent hyperintense lesions at white matter of bilateral cerebrum, and diminished sulci and fissures (A) accompanied by compressed lateral ventricles (B), herniation of para-hippocampal gyri (thick arrows), compressed choroidal fissures (arrowheads), diminished interpeduncular cistern (thin arrows), and deformity of the midbrain (C).

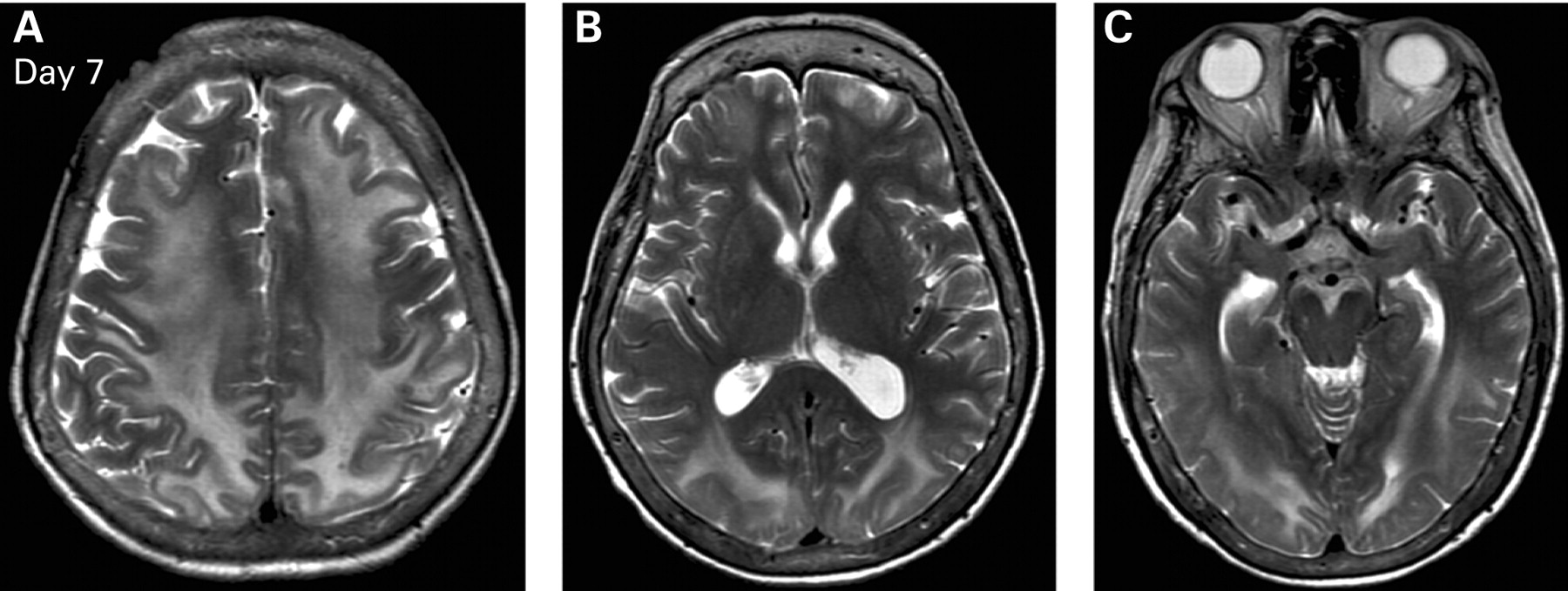
On day 7 after intense blood pressure control, the improvement of increased intracranial pressure manifested as ventricles returning to its normal size (B) and the relieving compression of brain stem (C). The brightness of white matter also subsided (A).

{kind=link}
{kind=link}
{kind=link}
On day 50, complete resolution of hyperintense lesions were demonstrated (A to C).
Patients with CKD are especially vulnerable to PRES because of frequent exposure to several of its possible causes including uraemia and hypertension. The spectrum of PRES can vary from seizures and coma to a mild headache. With timely blood pressure control and renal replacement therapy, the patient achieved total clinical recovery.
Acknowledgments
This work was supported by grants from the Ta-Tung Kidney Foundation, and the Mrs Hsiu-Chin Lee Kidney Research Fund, Taipei, Taiwan. For all authors, there was no conflict of interest to declare.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication