Article Text

Statistics from Altmetric.com
We report on a young man with large lumbar arteriovenous malformations presenting as high output heart failure and acute renal failure.
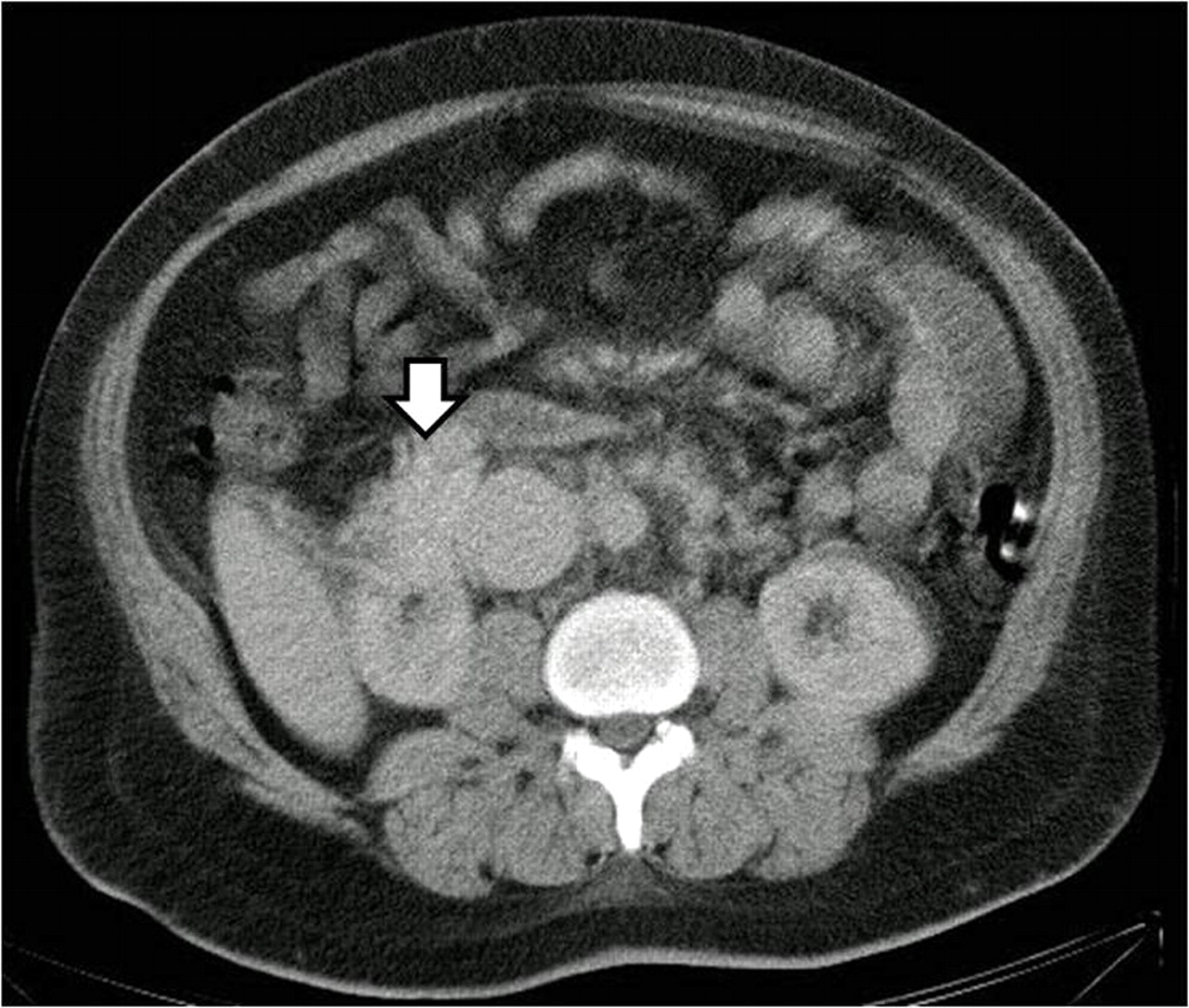
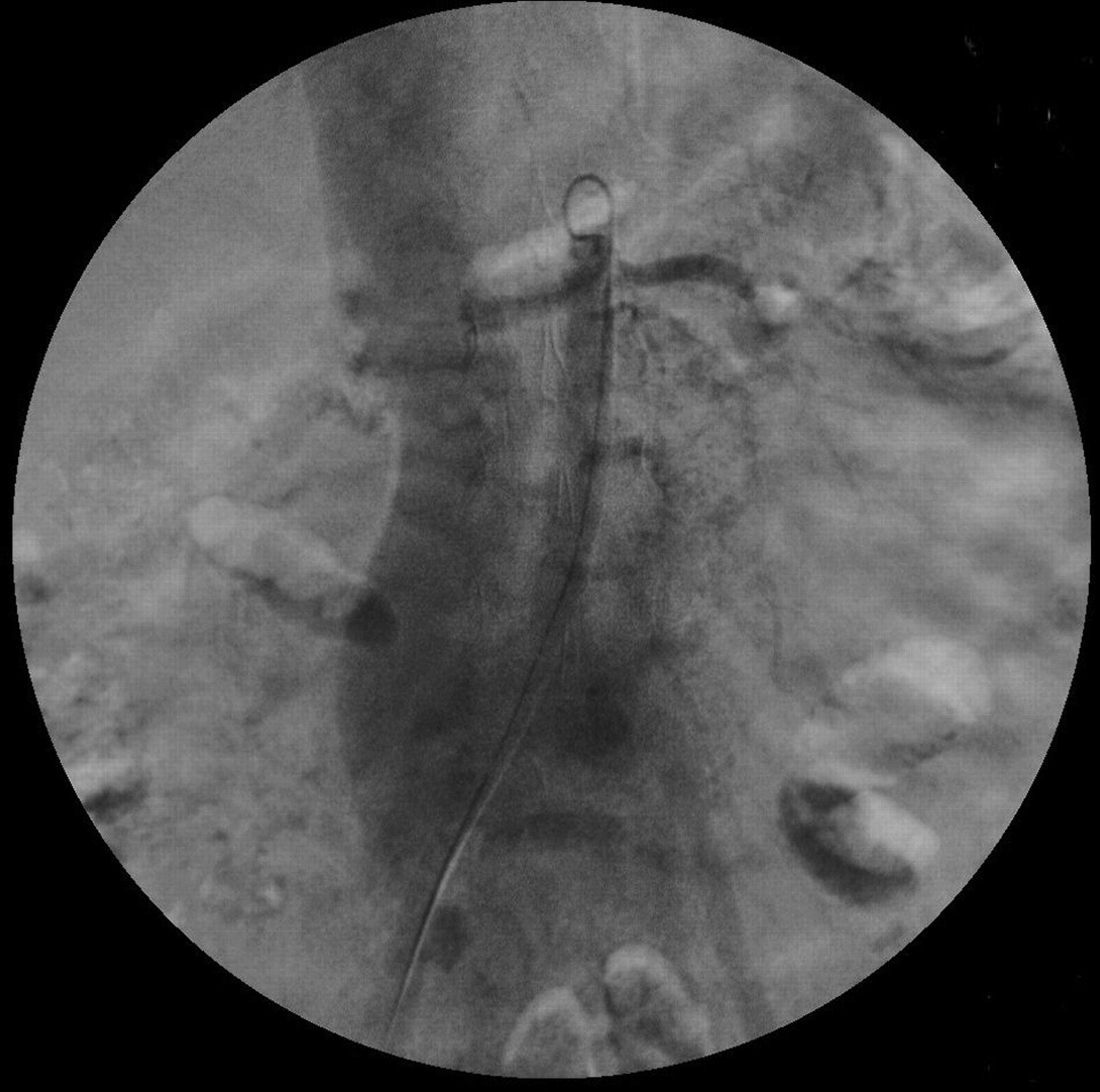
A 19-year-old obese male with hypertension, hyperlipidaemia, and gouty arthritis was admitted because of exertional dyspnoea, bilateral leg oedema, and scrotal swelling for 3 days. In the previous 2 years, he occasionally had exertional dyspnoea, especially when he had an upper respiratory infection. His weight was 131 kg, his height was 173 cm, and his blood pressure was 180/70 mm Hg. A grade 2/6 systolic murmur with an S3 was audible over the tricuspid area. His blood urea nitrogen was 24 mg/dl, creatinine 1.1 mg/dl, potassium 3.3 mEq/l. His chest x ray showed cardiomegaly and prominence of the pulmonary vasculature. The abdominal echo revealed liver congestion and splenomegaly. His heart failure was treated with captopril. Although his creatinine increased to 2.3 mg/dl after taking captopril, the renin–aldosterone values were unremarkable. The echocardiogram disclosed four-chamber dilatation, concentric hypertrophy, moderate pulmonary hypertension, and a left ventricular ejection fraction of 72%. Captopril renoscintigraphy and magnetic resonance angiography for secondary hypertension failed to reveal renal artery stenosis. His aortography and lumbar arteriography (fig 1) showed lumbar arteriovenous malformations (AVMs) and a normal renal artery. The contrast media flowed rapidly into the lumbar artery and the inferior vena cava in the early arterial phase. The clinical pictures mimic ischaemic stealing syndrome indicating that the lumbar AVMs may steal blood from the renal artery. The abdominal computed tomography showed a para-aortic hyperviscosity mass (fig 2). The AVMs were diffusely infiltrated in the abdominal cavity and abdominal wall.

{kind=link}
{kind=link}
The arrow indicates the para-aortic hyperviscosity mass.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication