Article Text

Statistics from Altmetric.com
Hepatic cysts are usually considered as benign lesions without symptoms. They can, however, become infected, ruptured and cause peritonitis. In the case presented here, a 77-year-old woman, not a carrier for hepatitis B or hepatitis C virus, and with previously asymptomatic polycystic liver disease, came to the emergency room with sudden onset of persistent right upper quadrant (RUQ) pain. Physical examination showed RUQ tenderness but with negative Murphy’s sign. The laboratory data showed leucocytosis with left shift and elevated C reactive protein. Liver enzymes were mildly elevated. Abdominal computed tomography (CT) scan (fig 1) suggested hepatic cyst rupture with peritonitis. Percutaneous drainage was attempted but failed. Septic shock developed soon after admission. The patient underwent emergency laparoscopic examination and pronounced turbid ascites with fibrin coating were noted (fig 2). The gall bladder was normal. Pus evacuation, partial excision with deroofing of the cystic wall, and drainage of the cavity and subphrenic space were performed. The uninfected cysts were operated on using the deroofing technique too. Antibiotics were used to treat Klebsiella pneumoniae, which was grown in blood culture media. The patient recovered gradually thereafter.

Multiple hepatic cysts with thickened inflamed wall (arrow) and perforation (arrowhead). The gall bladder was not involved.

{kind=link}
{kind=link}
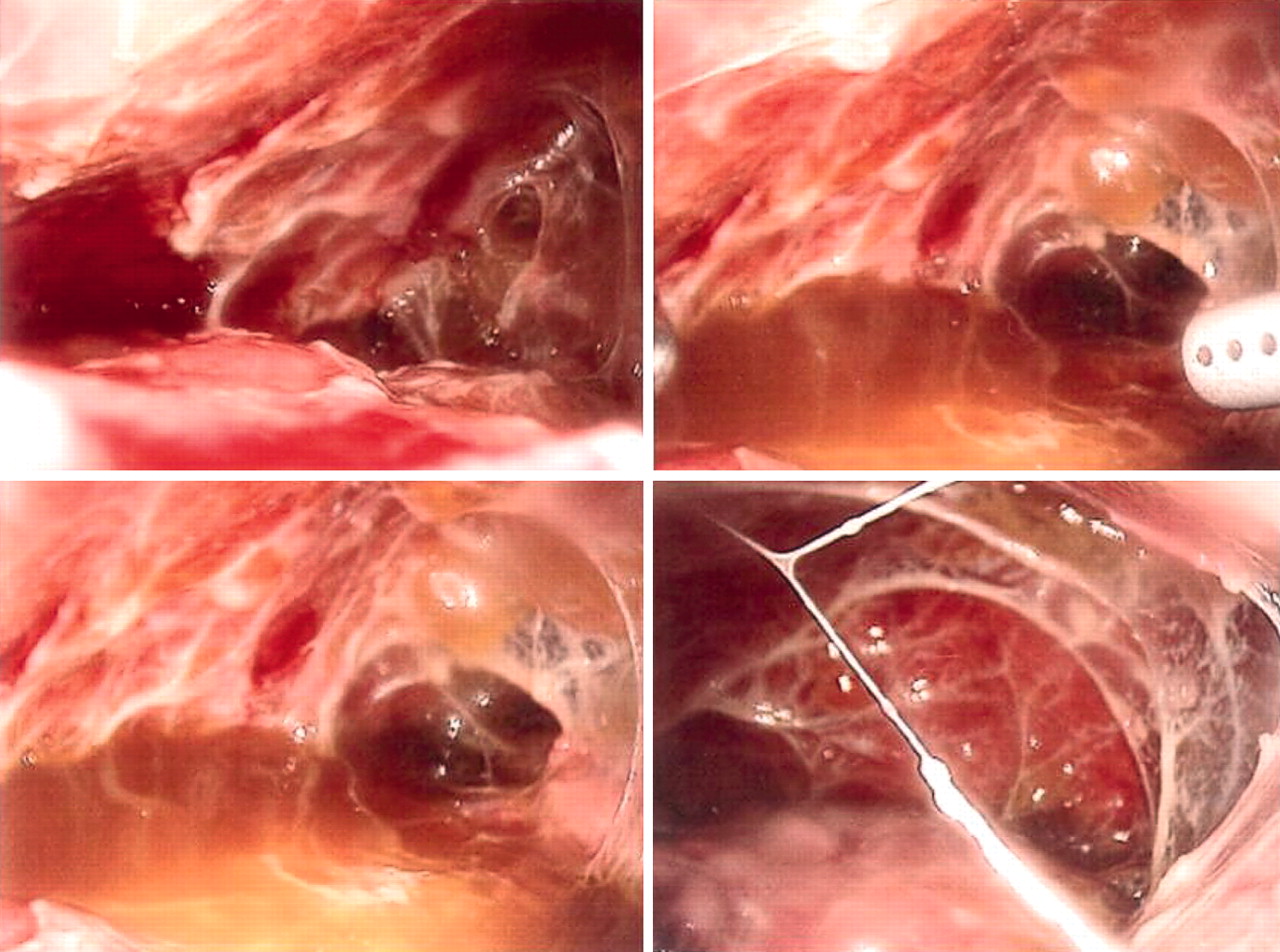
Laparoscopic views of the peritoneal cavity filled with turbid ascites and fibrin.
Risk factors for hepatic pyocysts include gut manipulation during abdominal operations, chronic haemodialysis, diabetes mellitus, and immunosuppressive therapy following organ transplantation.1 The organisms encountered most frequently are Escherichia coli, K pneumoniae, and Enterococcus species.2 Thickening of the wall is the characteristic finding, which can be localised through CT scan or scintigraphy (gallium-67 or indium-111 labelled leucocyte).3 Treatment of the pyocyst, if not perforated, includes percutaneous drainage and intravenous antibiotics. In those which rupture, resulting in peritonitis, urgent surgical intervention is mandatory. Peritoneal lavage with adequate drainage of residual pus in the cyst cured our patient.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication