Article Text

Summary
Aneurysms of tibial arteries are extremely rare. Here we report a case of a true posterior tibial artery aneurysm in a young patient without any associated pathology and discuss surgical and endovascular treatment. A young Caucasian male was admitted to our department for painful and pulsatile swelling of the right calf. Colour Doppler ultrasound scan visualised an aneurysmal dilation of the posterior tibial artery. The patient had no trauma to the area and denied other history of vascular disease. Angio-CT and angio-magnetic resonance imaging showed a larger aneurysm compared to ultrasound scan. We performed an embolisation of the aneurysm because of the risk of rupture, as distal collateral circulation ensured foot vascularisation. Endovascular treatment of aneurysms of small arteries seems to be a safe therapeutic and non-invasive choice, particularly in young patients in whom the presence of collaterals guarantees distal vascularisation.
Statistics from Altmetric.com
Background
A tibial artery aneurysm is a rare vascular lesion and the most frequent complications are aneurysm thrombosis, distal embolism and, rarely, rupture. The incidence of infrapopliteal and femoral artery aneurysms is well documented, but only a few cases of aneurysm of the posterior tibial artery have been reported in the literature. Common aetiological factors include trauma, collagen vascular pathology, fibromuscular dysplasia, infection, neurofibromatosis, polyarteritis nodosa and Behçet’s syndrome.
As reported in the English literature, treatment is indicated in symptomatic lesions or in a large aneurysm with a laminated thrombus. The most common treatment is surgical and includes saphenous vein bypass,1,2 ligation3,4 or end-to-end reconstruction.5 Endovascular treatment was reported in only one case, with coil embolisation of an aneurysm in a patient with Ehlers–Danlos syndrome.6
Case presentation
A 28-year-old Caucasian male was admitted to our department because of right calf pain which had begun during sleep. On examination we observed a pulsatile swelling of the right calf and colour Doppler ultrasound (CDU) scan revealed a 20 mm×25 mm diameter aneurysmal dilation of the posterior tibial artery with a mural thrombus. Family history for arterial aneurysm and connective tissue disorders was negative. No risk factors for atherosclerosis were present, and the patient’s medical history was otherwise unremarkable. He denied trauma to the area and had no other history of vascular disease. We found no possible causes for vasculitis. The patient underwent CT-angiography and magnetic resonance angiography that excluded the presence of dilations in other vascular beds but showed a larger aneurysm (22 mm×29 mm) compared to CDU. The patient complained of persistent pain in the right calf and a new CDU scan demonstrated a change in the appearance of the mural thrombus.
We used CDU to study the right lower leg vascularisation, and manually occluded the posterior tibial artery below the aneurysm. During the procedure the artery received retrograde flow by the pedal arch as far as the dilation, showing the presence of collateral circles and demonstrating the flow dominance of the anterior tibial artery.
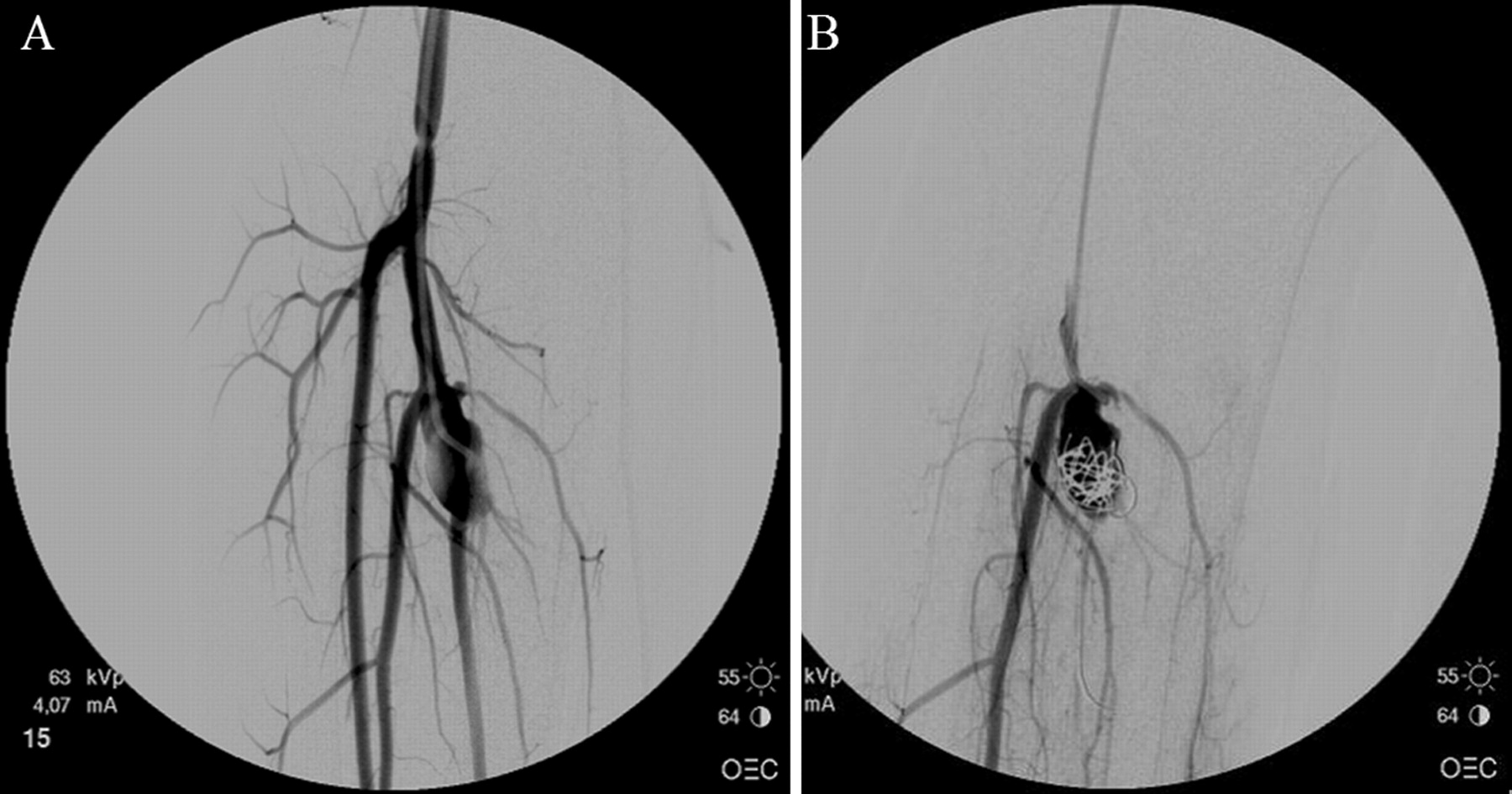
Under sedation, a single wall puncture of the femoral artery was performed and a 4F sheath and a 4F angiography catheter were introduced. The arteriogram visualised the presence of the aneurysm with patency of the posterior tibial artery. The anterior tibial artery provided the dominant flow to the foot while the peroneal artery was not involved in the aneurysm (figure 1A).

(A) Arteriogram showing a saccular aneurysm at the origin of the right posterior tibial artery. (B) Arteriography image showing embolisation of the aneurysm with occlusion of the right posterior tibial artery.
We performed coil embolisation of the aneurysm (figure 1B) with complete occlusion of the sac.
Outcome and follow-up
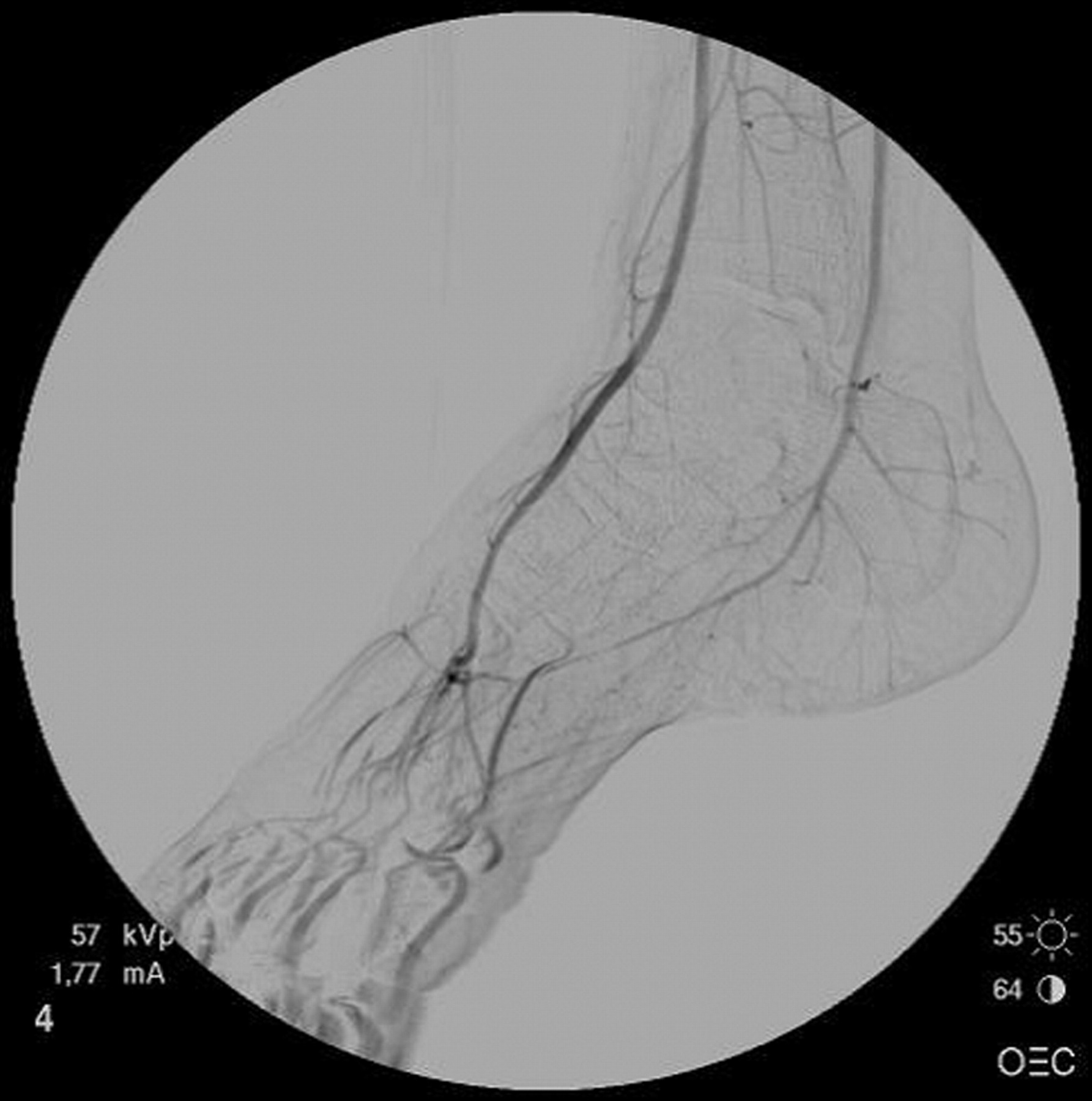
The patient’s post-operative course was uneventful. Because of collateral circles of the pedal arch (figure 2), the patient had no ischaemic signs, discomfort, pain, paresthesias or walking limitation. Follow-up 1 year later by CT and ultrasound scanning revealed complete absence of flow within the sac.
{kind=link}
{kind=link}
Arteriogram showing the posterior tibial artery in the distal portion that received flow via collateral circles.
Discussion
Aneurysms of the posterior tibial artery are rare with only a small number of case reports described in the literature (table 1). Trauma is the most common cause, while mycotic7 and collagenopathy-related causes6 are infrequent.
Posterior tibial artery aneurysms described in the literature
The therapeutic management of a tibial artery aneurysm depends on the presence or absence of symptoms. Small and asymptomatic aneurysms may be safely kept under observation.
The options for surgical treatment include ligation and exclusion of the aneurysm if there is no resultant ischaemia of the foot, or end-to-end direct reconstruction, resection and bypass.11
Endovascular treatment should be reserved for selected patients with symptomatic aneurysms6 or when open repair is either not feasible or difficult.12
In our case, as the dilation was close to the peroneal–posterior tibial bifurcation, open repair or endovascular stenting was not advisable. The persistence of pain and the change in mural thrombus appearance suggested that the dilation could evolve into rupture of the aneurysm.
Instead of exploring, resecting and bypassing the artery, we chose to perform a coil embolisation of the aneurysm, as the anterior tibial and peroneal artery were not involved in the aneurysm and foot vascularisation was ensured by distal collateral circulation. After embolisation, the posterior tibial artery received flow via collateral circles, and the patient had no signs of ischaemia in the lower leg. Follow-up confirmed a good outcome.
Particularly in selected patients, endovascular treatment of tibial artery aneurysms is a useful alternative to a surgical approach.
Learning points
-
A tibial artery aneurysm is a rare vascular lesion, especially in young patients.
-
Management of tibial artery aneurysms depends on the presence or absence of symptoms; small and asymptomatic aneurysms may be observed safely.
-
Endovascular treatment of tibial artery aneurysms is a useful alternative to a surgical approach in selected patients.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.