Article Text

Statistics from Altmetric.com
A 70-year-old man presented with a 6 month history of grade II exertional chest tightness. At peak exercise on treadmill he developed borderline ST segment depression in lead V4. Cardiac catheterisation showed angiographically minor stenosis in the proximal left anterior descending artery (fig 1). However, on intravascular ultrasound, there was at least moderate atheroma burden in this segment, although the lumen was well preserved due to positive remodelling (fig 2). This is a striking example of the Glagov phenomenon (first described in 1987)1 whereby positive remodelling of the arterial wall enables lumen diameter to be maintained up to a plaque burden of 40–45% diameter, but above 40–45%, reduction in lumen occurs due to inability of the artery to expand further.

Angiographically minor stenosis in the proximal left anterior descending artery.
{kind=link}
{kind=link}
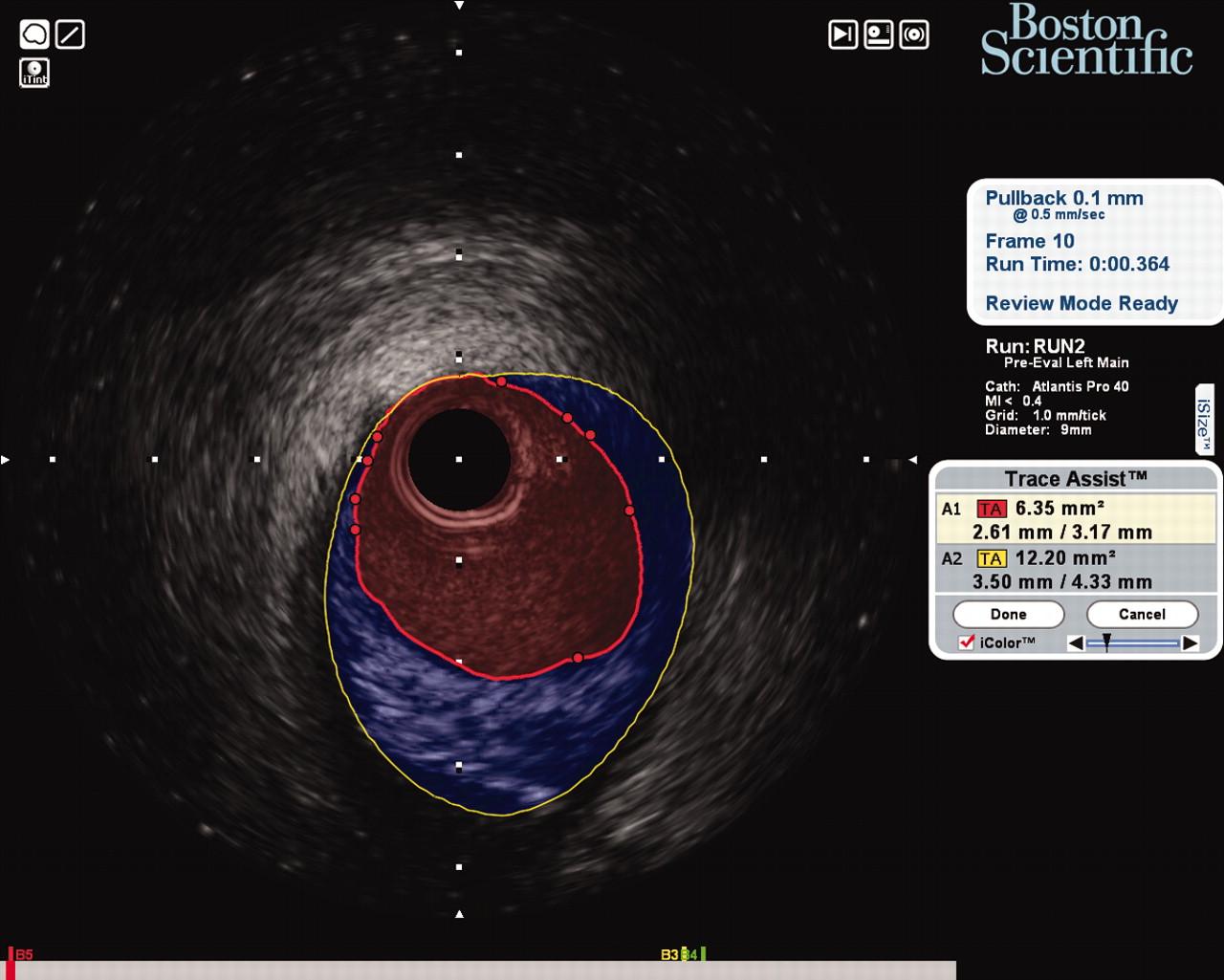
Intravascular ultrasound of the same segment showing at least moderate atheroma burden (blue), with preservation of the lumen (red) due to positive remodelling—the Glagov phenomenon.
REFERENCES
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication