Article Text

Statistics from Altmetric.com
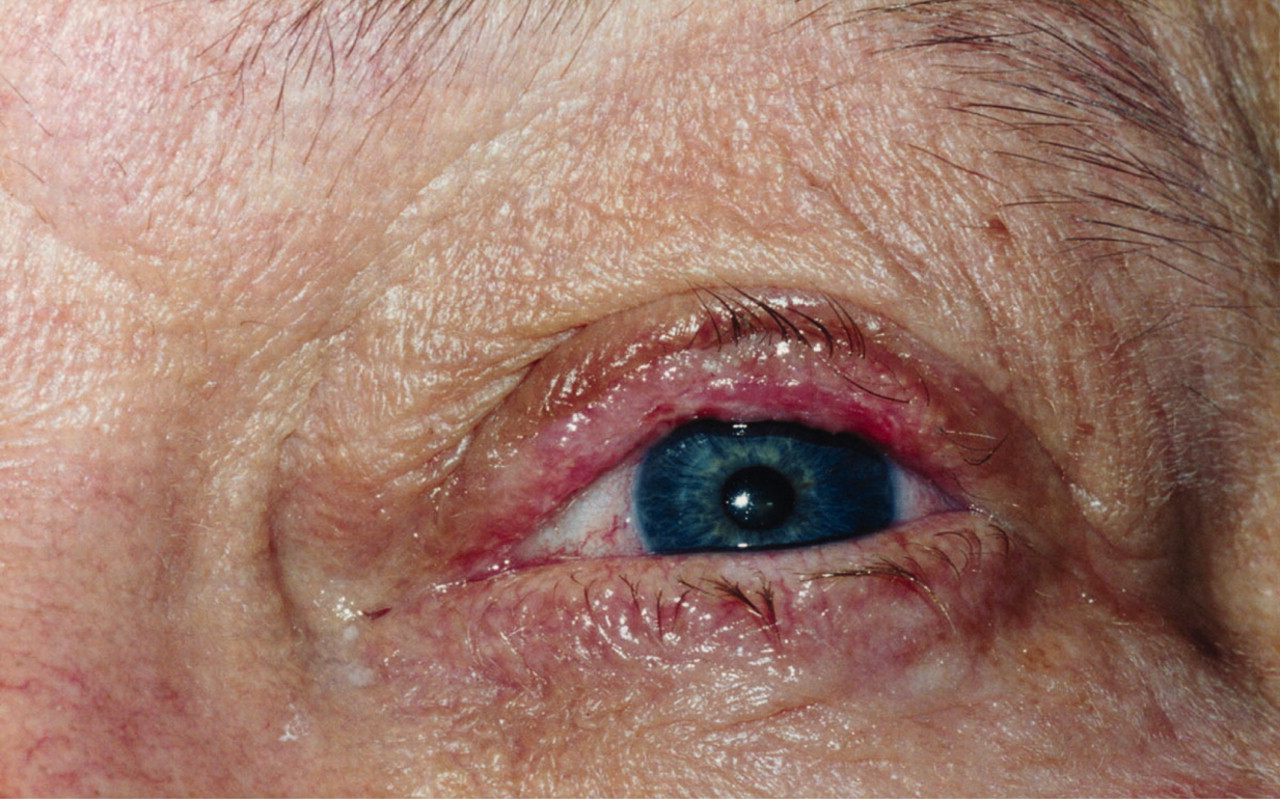
A man in his 60s presented with dry eyes and progressive deterioration in vision bilaterally over a 2-year period. He was treated a number of times presumptively for conjunctivitis with topical antibiotics. Upon referral to an ophthalmologist, physical examination revealed the presence of conjunctival scarring with loss of the fornix, symblepharon (adhesion between conjunctival surfaces of the lid and globe), entropion (lid inversion due to conjunctival scarring) and trichiasis (aberrant lashes causing abrasion of the cornea) (figs 1–3). The conjuctival signs were readily apparent when the patient was instructed to gaze laterally and vertically. There was no clinical involvement of other mucosal or skin surfaces. A conjuctival biopsy revealed subepithelial separation at the level of the basement membrane with stromal infiltration of lymphocytes and dense fibrous tissue. Direct immunofluoresence demonstrated the characteristic linear deposits of IgG along the basement membrane (fig 4). Local therapies that were implemented included lubricants, punctual occlusion and destruction of aberrant lash follicles. He also required systemic immunosuppressive therapy with oral prednisone, initially given at 0.5 mg/kg/day. His visual acuity then gradually improved and after 2 years is maintained at a dose of 0.1 mg/kg/day.

Lid deformities with ectropion (lid eversion) of the upper lid and entropion (lid inversion) of the lower lid.

Scarring of the conjunctival surface with trichiasis (aberrant lashes) resulting in corneal abrasion.

Symblepharon formation (adhesion of the conjuctival surfaces of lid and globe) resulting in narrowing of the formix.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
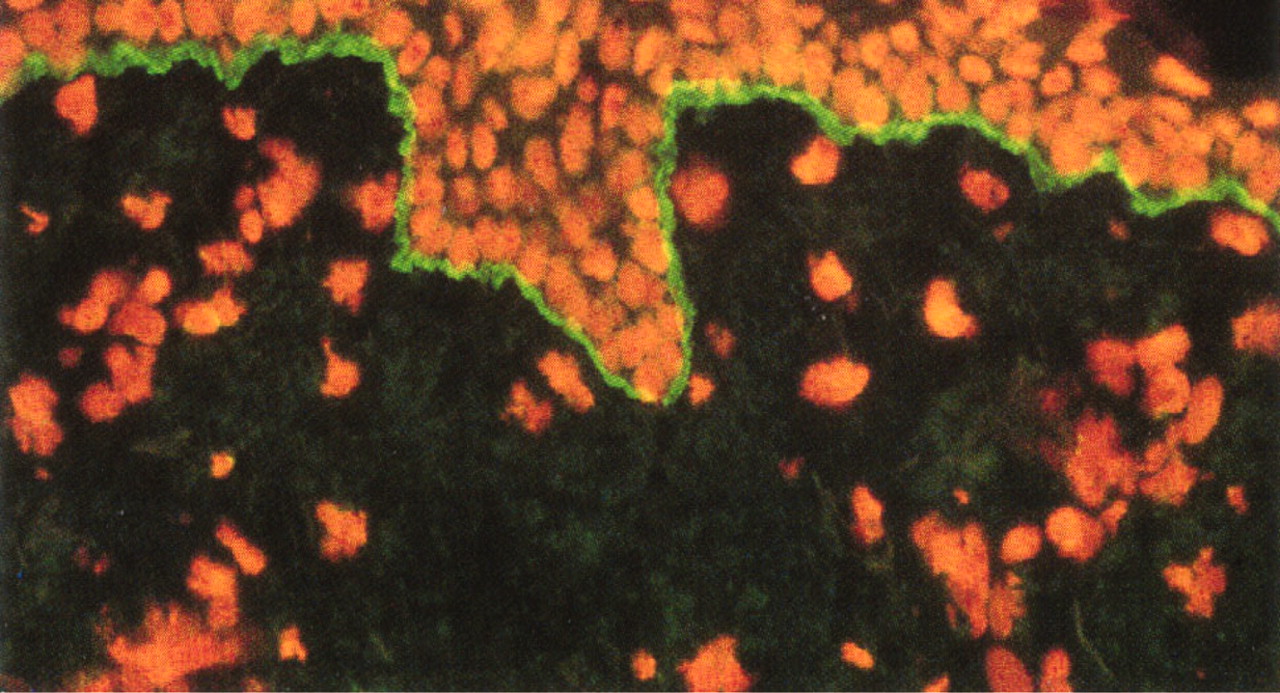
Direct immunofluorescence of a conjunctival biopsy demonstrating linear deposition of IgG along the basement membrane zone.
The diagnosis of ocular mucous membrane pemphigoid is often missed or delayed and chronic changes can lead to reduction in vision from corneal scarring and ulceration and dry eyes from lacrimal duct occlusion.1 Early diagnosis through recognition of ocular cicatrisation supported by the demonstration of autoimmune-mediated damage to the basement membrane by direct immunofluoresence enables local and systemic therapies to be more effective in ameliorating long term complications.2,3
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.