Article Text

Abstract
A previously healthy Japanese woman in her 20s was admitted to our hospital with a 2-week history of fever (39.0°C) and a 1-week history of painful cervical lymphadenopathy. The day before fever onset, she had received her first Pfizer-BioNTech SARS-CoV-2 vaccine in her left arm. She had previously been treated with empirical antibiotics with no improvement. Physical examination revealed painful lymphadenopathy in both posterior cervical regions. CT showed symmetrical lymphadenopathies in the neck, supraclavicular, axillary and inguinal regions as well as hepatosplenomegaly. We suspected lymphoma and performed a lymph node biopsy in the right inguinal region, which revealed necrotising histiocytic lymphadenitis. The patient was, therefore, diagnosed with Kikuchi-Fujimoto disease (KFD). She improved after the corticosteroid therapy. This report highlights the importance of including KFD as a differential diagnosis of lymphadenopathy after SARS-CoV-2 vaccination. Additionally, lymph node biopsy is helpful for diagnosing KFD because it rules out other entities.
- Vaccination/immunisation
- COVID-19
- Medical education
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Kikuchi-Fujimoto disease (KFD), also known as histiocytic necrotising lymphadenitis, is a relatively rare disease.1 The aetiopathology of KFD is unclear; however, infection, autoimmunity and/or genetic predisposition are thought to be involved.2 This condition was initially reported in Asians but has now been reported worldwide in patients of various ethnic backgrounds. KFD is characterised by cervical (most common), axillary and/or supraclavicular lymphadenopathy with tenderness and is usually accompanied by fever; thus, it may closely resemble infectious, autoimmune or neoplastic disease.2 The differentiation can be broad, especially when extranodal involvement is present.3
Given that the SARS-CoV-2 vaccine was developed based on the novel idea of using messenger RNA (mRNA),4 the potential for in vivo reactions with immune mechanisms, including adverse effects, has attracted considerable attention.5 In the ongoing COVID-19 pandemic, the lymphadenopathy seen in some individuals following the SARS-CoV-2 vaccination is often reactive.6 Several reports have described KFD-induced lymphadenopathy following SARS-CoV-2 vaccination.7–12
Clarifying the possible relationship between vaccines and autoimmune diseases is difficult because of the lack of specificity and the absence of clear diagnostic criteria.13 The two hypothesised mechanisms for the development of autoimmune diseases following vaccination are molecular mimicry,14 wherein vaccines trigger an immune response against self-antigens, and bystander activation,15 wherein vaccines release self-antigens from host tissues and activate antigen-presenting cells and dormant autoreactive T-helper cells.
Case presentation
A previously healthy Japanese woman in her 20s presented to our general outpatient department with a chief report of fever and painful cervical lymphadenopathy. The clinical course is shown in figure 1. She had received her first dose of the Pfizer-BioNTech SARS-CoV-2 vaccine 2 weeks earlier and developed a fever the following day. One week before her visit, she developed swelling and pain in her neck, which was diagnosed as a bacterial infection by her family doctor and treated empirically with levofloxacin. However, her condition did not improve.
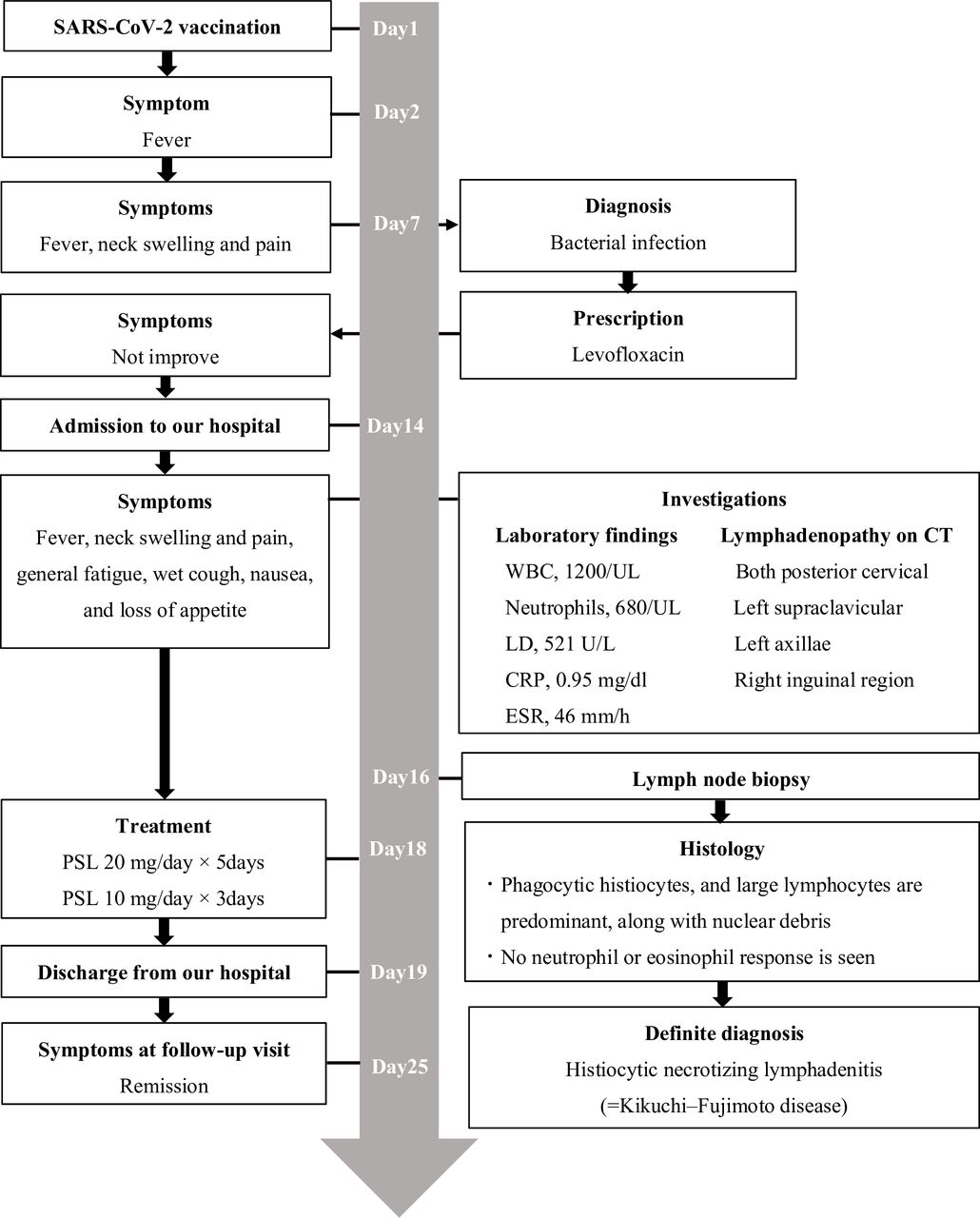
Timeline of clinical progress. CRP, C reactive protein; ESR, erythrocyte sedimentation rate; LO, lactate dehydrogenase; PSL, prednisolone; WBC, white blood cells.
On arrival, the patient reported of fever, neck swelling and pain, general fatigue, a wet cough, nausea and loss of appetite but did not report night sweats, weight loss or hair loss. She was a non-smoker and did not consume alcohol. She denied any history of contact with someone who was unwell, recent travel or contact with animals. She had a partner but had not recently been sexually active. She had no significant family history. She was febrile with a body temperature of 39°C. Her other vital signs were normal. Physical examination revealed firm, tender and mobile lymph nodes that measured up to 1 cm in size in the bilateral posterior cervical regions, the left supraclavicular region, the bilateral axillae and the right inguinal region. No skin rash, oral ulceration or arthralgia was observed. Cardiovascular, pulmonary and abdominal examination findings were unremarkable.
Investigations
Laboratory investigations (table 1) revealed leucopenia (white blood cells, 1.2 ×109/L; neutrophils, 0.68×109/L; lymphocytes, 0.41×109/L; monocytes, 0.1×109/L) and an elevated lactase dehydrogenase concentration (521 U/L; reference range, 124–222 U/L). The erythrocyte sedimentation rate was increased at 46 mm/hour (reference range, 0–30 mm/hour) and the C reactive protein (CRP) concentration was 0.95 mg/dL (reference range, 0.00–0.30 mg/dL). Her blood urea nitrogen concentration, electrolyte concentrations and liver function test results were normal. Serological tests for the hepatitis B virus, hepatitis C virus, herpes virus, Epstein-Barr virus and cytomegalovirus were negative. Tests for HIV and human parvovirus B19 were not performed. Blood cultures showed no bacterial growth after 48 hours. Her immunoglobulin G, A and M levels; complement C3 and C4 concentrations and antinuclear antibody titre were normal. A PCR test for SARS-CoV-2 was negative.
Comparison of clinical findings between the present case and previous reports
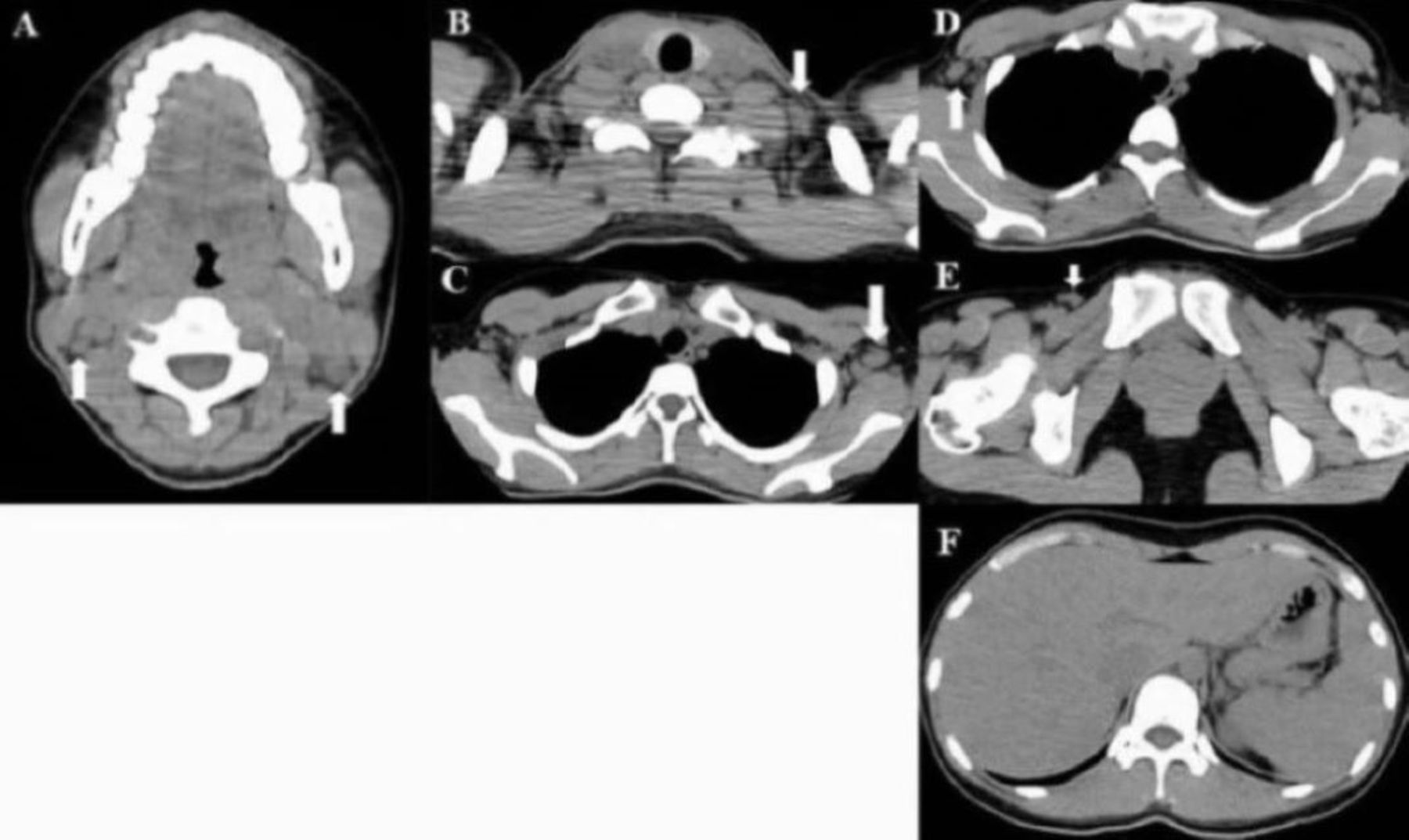
CT showed lymphadenopathy in the bilateral cervical regions (figure 2A), left supraclavicular fossa (figure 2B), bilateral axillae (figure 2C,D) and right inguinal region (figure 2E) as well as hepatosplenomegaly (figure 2F). The patient was admitted for further examination and treatment. We performed a right inguinal lymph node biopsy. Both large and small foci and fusion of histiocytes and lymphocytes were seen from the paracortex to the cortex of the lymph node (figure 3A). Apoptosis and nuclear debris were observed in the central part of the lesion, and abundant histiocytes were phagocytosing the debris (figure 3A). No neutrophils or eosinophils, granulomas or inclusion bodies were seen. Immunohistochemical staining showed increased numbers of CD3+, CD4+ and CD8+T cells and CD68+ histiocytes but no CD20+B cells (figure 3B–F).

CT findings. CT scans showed lymphadenopathy in the (A) bilateral cervical regions, (B) left supraclavicular fossa, (C, D) bilateral axillae and (E) right inguinal region (white arrow) as well as (F) hepatosplenomegaly.

{kind=link}
{kind=link}
{kind=link}
Histopathologic findings. The patient underwent an excisional right inguinal lymph node biopsy. (A) Large and small foci and fusion of histiocytes and lymphocytes were seen from the paracortex to the cortex of the lymph node. Apoptosis and nuclear debris were observed in the central part of the lesion, and abundant histiocytes were phagocytosing this debris. No neutrophils or eosinophils were seen. Immunostaining showed an increase in (B) CD3+, (C) CD4+, and (D) CD8+ T cells and (E) CD68+ histiocytes. (F) No CD20+ B cells were seen. Histopathological features of the lymph nodes of patients with Kikuchi-Fujimoto disease include numerous phagocytic histiocytes, lymphocytes, marked nuclear debris and apoptosis. Neutrophils and eosinophils are generally absent. Immunohistological findings predominately comprise CD68+ histiocytes, CD4+ T cells and CD8+ T cells, with few B cells. These findings confirmed histiocytic necrotising lymphadenitis in the present case.
Differential diagnosis
When a patient presents with generalised lymphadenopathy, fever and hepatosplenomegaly, the principal differential diagnoses are infection, autoimmune disease and malignancy. When supraclavicular lymphadenopathy and hepatosplenomegaly are present, malignancy should be excluded as rapidly as possible with prompt evaluation to ensure appropriate therapeutic management. With respect to infection, the main differential diagnoses in our patient’s age group are infectious mononucleosis, tuberculosis and toxoplasmosis, whereas the main differential for autoimmune disease is systemic lupus erythematosus (SLE). It is also essential to rule out HIV and syphilis in such cases. Furthermore, in view of the worldwide use of the SARS-CoV-2 vaccine, clinicians should also consider reactive lymphadenopathy following vaccination as another differential.16
In this case, no malignant cells were found in the pathological examination. Reed-Sternberg cells, which are the hallmark of Hodgkin’s disease, were also absent. Viral serology and blood culture were negative, and the histological appearance and cellular composition of the lymph nodes showed no evidence of an infectious process. There was no non-caseating granulomas characteristic of sarcoidosis. Immunohistochemical examination showed that the lymphocytes mostly comprised CD3+, CD4+ and CD8+T cells and that the histiocytes were CD68+, which is consistent with histiocytic necrotising lymphadenitis.1 Ultimately, the patient was diagnosed with KFD.
Although KFD has been associated with autoimmune disorders, including SLE, mixed connective tissue disease, antiphospholipid antibody syndrome and scleroderma,17 none of the diagnostic criteria for any of these diseases was met in this case.
Treatment
The patient’s symptoms did not improve by treatment with a non-steroidal anti-inflammatory drug. Therefore, her treatment was switched to prednisolone at 20 mg/day for 5 days, followed by 10 mg/day for 3 days.
Outcome and follow-up
Her symptoms improved rapidly after starting prednisolone. Her leucocyte count and lactase dehydrogenase concentration had improved to baseline levels by 1-week follow-up visit. The patient provided informed consent for treatment and publication of this case report, and she approved the use of her clinical data.
Discussion
We encountered a rare case of KFD following SARS-CoV-2 vaccination. In general, lymphadenopathy following SARS-CoV-2 vaccination in the ipsilateral neck and axilla is mainly painless, reactive and transient. Although the association between the SARS-CoV-2 vaccine and KFD has not yet been established, clinicians should consider KFD as a differential diagnosis when patients present with painful lymphadenopathy. The differential diagnoses varied widely in the present case because the patient had generalised lymphadenopathy and extranodal involvement, unlike patients described in previous reports. When painful lymphadenopathy does not improve spontaneously and/or with initial treatment (eg, antimicrobial prescription), as in our case, lymph node biopsy is helpful for diagnosis and management.
Similar cases of KFD following the SARS-CoV-2 vaccine have been reported.7–12 Table 1 compares the clinical findings in previous cases of KFD following SARS-CoV-2 vaccination with those in our patient. All patients were adolescents or young adults with a male:female ratio of 3:4. One patient was Middle Eastern,7 one European9 and one African12; however, most were Asian.8 10 11 All patients presented with fever and painful lymphadenopathy in the neck, supraclavicular region or axilla after vaccination; four developed the symptoms after the first vaccination7 8 and three developed symptoms after the second vaccination.9 10 Most vaccines were mRNA vaccines7–9; only one was an inactivated vaccine.10 The site of lymphadenopathy in most patients was ipsilateral to the vaccine administration site. Hepatosplenomegaly was observed as an extranodal lesion in one patient.11 Our patient had symmetrical systemic lymphadenopathy with hepatosplenomegaly as extranodal involvement. The majority (60%–90%) of patients with KFD present with painful tender posterior cervical lymphadenopathy, often involving the axillary and supraclavicular lymph nodes.1 However, systemic lymphadenopathy is reported less often (in 1%–22% of cases).1 Furthermore, hepatosplenomegaly as a form of extranodal involvement is rare, being reported in <5% of cases.17 Extranodal involvement can also occur in the skin, bone marrow and liver.18–20 The patient in case 1 (see table 1) had elevated liver enzymes and thrombocytopenia and may have had hepatosplenomegaly due to liver disease. Considering the previous reports, clinicians should consider KFD as a differential diagnosis when examining patients presenting with painful lymphadenopathy following SARS-CoV-2 vaccination and should note the distribution of lymphadenopathy and its association with extranodal involvement.
Different vaccine manufacturers have reported differences in the occurrence of lymphadenopathy. The Pfizer-BioNTech SARS-CoV-2 vaccine trial showed that ipsilateral axillary and supraclavicular lymphadenopathy occurred at a rate of 0.3%.21 The Centers for Disease Control and Prevention reported that for both Pfizer22 and Moderna,23 lymphadenopathy occurs in the ipsilateral arm and neck region within 2–4 days following vaccination. The mean duration of lymphadenopathy after the Moderna vaccine is approximately 10 days, whereas the median duration after the Pfizer vaccine is 1–2 days. In the present case, lymphadenopathy appeared 1 week after vaccination, and in previous reports appeared at 17–90 days.7–12 These findings suggest that lymphadenopathy in patients with KFD may appear later than in patients with reactive lymphadenopathy. When lymphadenopathy persists for more than 10 days, clinicians should consider causes other than reactive lymphadenopathy.
Clinicians should consider KFD as a differential diagnosis in patients with fever, painful lymphadenopathy and hepatosplenomegaly following SARS-CoV-2 vaccination. Although the key clinically diagnostic features of KFD are posterior cervical lymphadenopathy with tenderness and fever, KFD can also present with systemic lymphadenopathy or extranodal involvement. Clinicians should also note that KFD may mimic various infectious lymphadenopathies, autoimmune lymphadenopathies (mainly SLE lymphadenopathy) and malignant diseases (lymphomas and metastases). In differentiating infection, infectious agents can be identified by immunohistochemical and other specific stains. Occasionally, clinicians must distinguish between KFD and lymphadenitis caused by infectious mononucleosis. Hodgkin and Reed-Sternberg-like cells may be present in infectious mononucleosis,24 but positive Epstein-Barr virus-coding RNA in situ hybridisation can help to resolve any diagnostic dilemma.25 In differentiating autoimmune disease, SLE-associated lymphadenopathy is the most challenging differential diagnosis to resolve, sometimes being histologically and immunochemically indistinguishable from KFD.26 Moreover, KFD can precede, follow or coincide with SLE.26 Given the similarity between SLE-associated lymphadenopathy and KFD, clinicians should always include SLE as a differential diagnosis and distinguish between the two diseases clinically and by laboratory investigations. In differentiating malignant disease, KFD is easily confused with lymphoma.27 Ultrasound and CT reportedly cannot differentiate KFD-associated lymphadenopathy from lymphoma or metastatic disease.28 However, myeloperoxidase positivity is a helpful clue to the presence of histiocytes when differentiating malignant cells.29 We performed a lymph node biopsy on our patient because we suspected lymphoma. A biopsy is useful when the differential diagnosis is broad, but small biopsies and needle biopsies may not provide a clear picture of the pattern of disease; incisional or excisional biopsy specimens are preferred.1
Laboratory and histological findings have a supportive role in reaching the correct diagnosis. Blood tests in our patient revealed transient leucopenia, elevated lactase dehydrogenase and CRP concentrations and a high erythrocyte sedimentation rate.1 Some patients present with mild anaemia, a mildly increased erythrocyte sedimentation rate and an elevated CRP concentration. Other reported findings include leucopenia (especially granulocytopenia, found in 20%–58% of patients), leukocytosis (found in 2%–5% of patients) and atypical lymphocytes in peripheral blood (found in up to one-third of patients). Other laboratory abnormalities, such as elevated serum concentrations of lactate dehydrogenase and aminotransferases, are also observed in some patients. Histologically, T-cell-mediated hyperimmunity1 and activation of CD8+T cells influence the pathogenesis of both KFD1 and post-COVID-19 infection.30 Two postulated mechanisms of autoimmune disease development following vaccination are molecular mimicry,14 wherein vaccines trigger an immune response against self-antigens, and bystander activation,15 wherein vaccines release self-antigens from host tissues and activate antigen-presenting cells and dormant auto-reactive T-helper cells. The present case suggests that molecular mimicry by the SARS-CoV-2 vaccine may be involved in the T-cell-mediated mechanism. KFD is a self-limiting disease and usually resolves in a few months; therefore, no specific treatment is required, and relief of symptoms is the mainstay of treatment. Considering the high likelihood that immunity is involved in the aetiology of KFD, clinicians should consider glucocorticoids31 if symptoms do not improve.
Based on our experience, vaccination can be a cause of lymphadenopathy. We have summarised and updated the literature on lymphadenopathy caused by any vaccine, including live and inactivated vaccines and toxoids (table 2). How vaccines lead to the development of KFD is unknown; however, viruses and other antigens in vaccines, as well as mRNA, might lead to an abnormal immune response in a vaccine recipient and cause them to develop KFD. Clinicians should be aware of the possibility of KFD developing after vaccination for viral species, including the SARS-CoV-2 vaccine. Further research on the association between vaccine types and KFD is needed.
Summary of vaccine-related lymphadenopathy following vaccination, including SARS-CoV-2 mRNA vaccine
Conclusion
Clinicians can reasonably suspect KFD when a patient develops fever and painful lymphadenopathy after vaccination for viral species, including the SARS-CoV-2 vaccine, regardless of the side on which the vaccine was administered. The critical features for a clinical diagnosis of KFD are fever and posterior cervical lymphadenopathy with tenderness. Considering that the differential diagnosis of KFD is broad, clinicians need to differentiate infectious lymphadenopathies, autoimmune diseases (mainly SLE lymphadenopathy) and malignant diseases (lymphoma and metastasis). When painful lymphadenopathy does not improve spontaneously and/or with initial treatment (eg, antimicrobial prescription), lymph node biopsy should be considered as a diagnostic tool for KFD because it can rule out other pathologies. In the era of the COVID-19 pandemic and global vaccination programmes, although no causal association between the SARS-CoV-2 vaccine and KFD has been established, clinicians should be aware of KFD as an uncommon adverse effect of the SARS-CoV-2 vaccine and should include KFD as a differential diagnosis for patients who present with painful posterior cervical lymphadenopathy and fever following SARS-CoV-2 vaccination.
Patient’s perspective
After receiving the COVID-19 vaccine, I had a fever of 38℃. I thought it was just ‘one of the side effects. However, a week later, I felt something wrong with my neck and visited the hospital where I was vaccinated. The doctor then evaluated that it was a problem-less side effect. I thought, ‘if these symptoms are side effects, I do not want to be vaccinated again’, so I went to another hospital. After the doctor’s examination, I was immediately admitted to the hospital to explore the cause. I was anxious, but the kindness of the doctor and nurses soothed me. After the biopsy, I sometimes had trouble sleeping because of the pain, but I am now pain-free and able to lead an everyday daily life. Kikuchi-Fujimoto disease is unfamiliar. However, I hope this case will help medical science develop and support patients like me.
Learning points
The SARS-CoV-2 vaccine can trigger Kikuchi-Fujimoto disease (KFD).
Symptoms of KFD mimic those of other serious diseases, such as infection, autoimmune disease, malignancy, and even reactive lymphadenopathy following SARS-CoV-2 vaccination.
When painful lymphadenopathy does not improve spontaneously and/or with initial treatment (eg, antimicrobial prescription), lymph node biopsy should be considered for diagnosing KFD.
The clinician should include KFD as a differential diagnosis in patients with painful lymphadenopathy and fever following SARS-Cov-2 vaccination.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors KI wrote this case report. EK and SA edited and reviewed the manuscript. KK edited and supervised the information.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.