Article Text

Statistics from Altmetric.com
Description
A 36-year-old man presented to our ophthalmology clinic with redness, pain and progressively diminishing vision in the left eye for 2 days. He had sustained a blunt trauma from a fist punch to the left side of his face, 6–7 hours before the appearance of first symptoms. His best corrected visual acuity was 20/50 in the left eye and 20/20 in the right eye. The intraocular pressure was 15 mm Hg in both eyes. The slit lamp biomicroscopy of the left eye showed white axial opacities in the form of five distinct quadrangular ‘petals’, giving it a characteristic rosette pattern (figure 1). The posterior segment examination, performed after dilation, was essentially normal in both eyes (figure 2). The patient underwent cataract extraction surgery with intraocular lens implantation (figure 3). One week after the surgery, the patient’s distance and near visual acuity were recorded to be 20/20 and N6 with +2D, respectively.

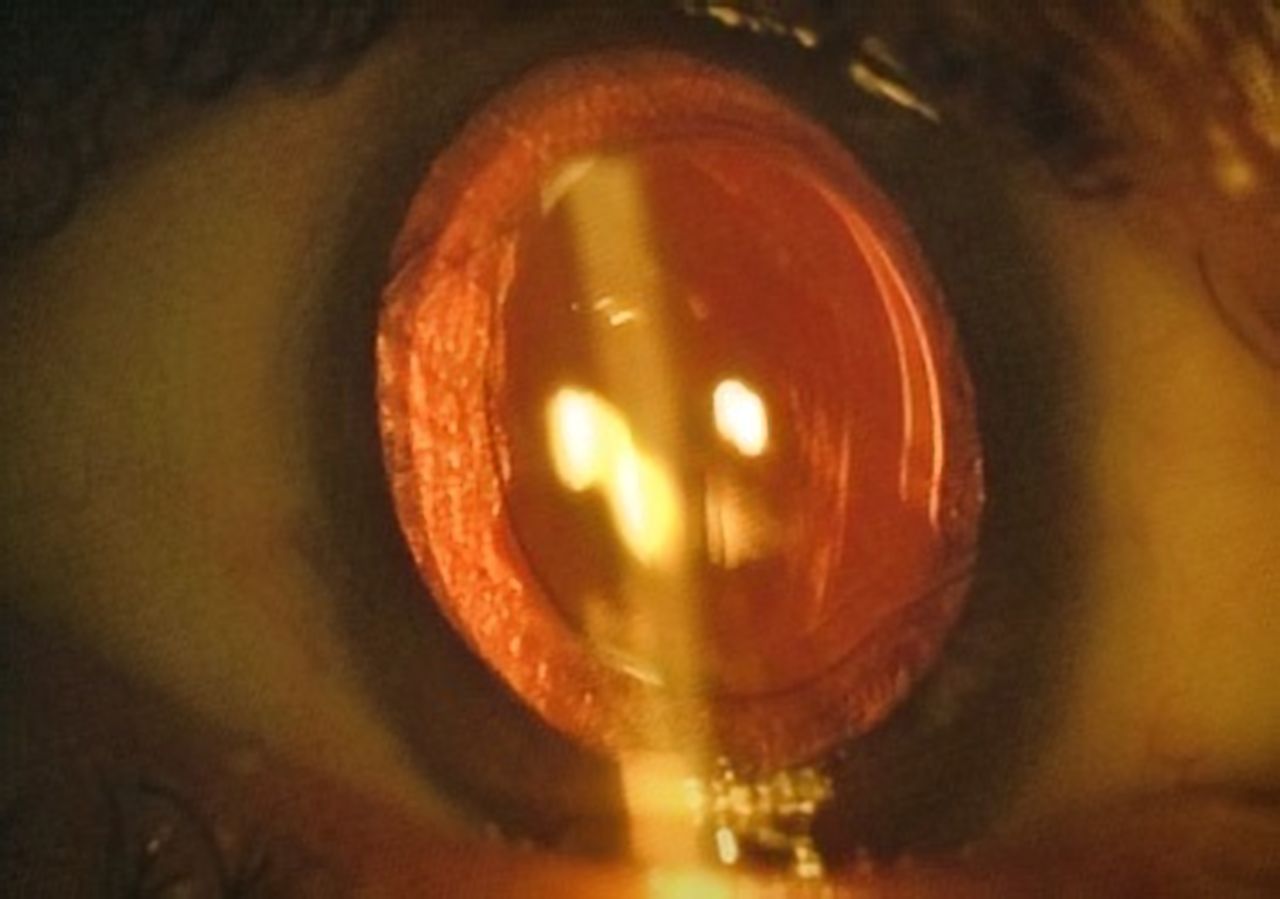
The patient’s slit lamp examination showed white axial quadrangular petal-shaped opacities arranged in a floral pattern in the left eye.

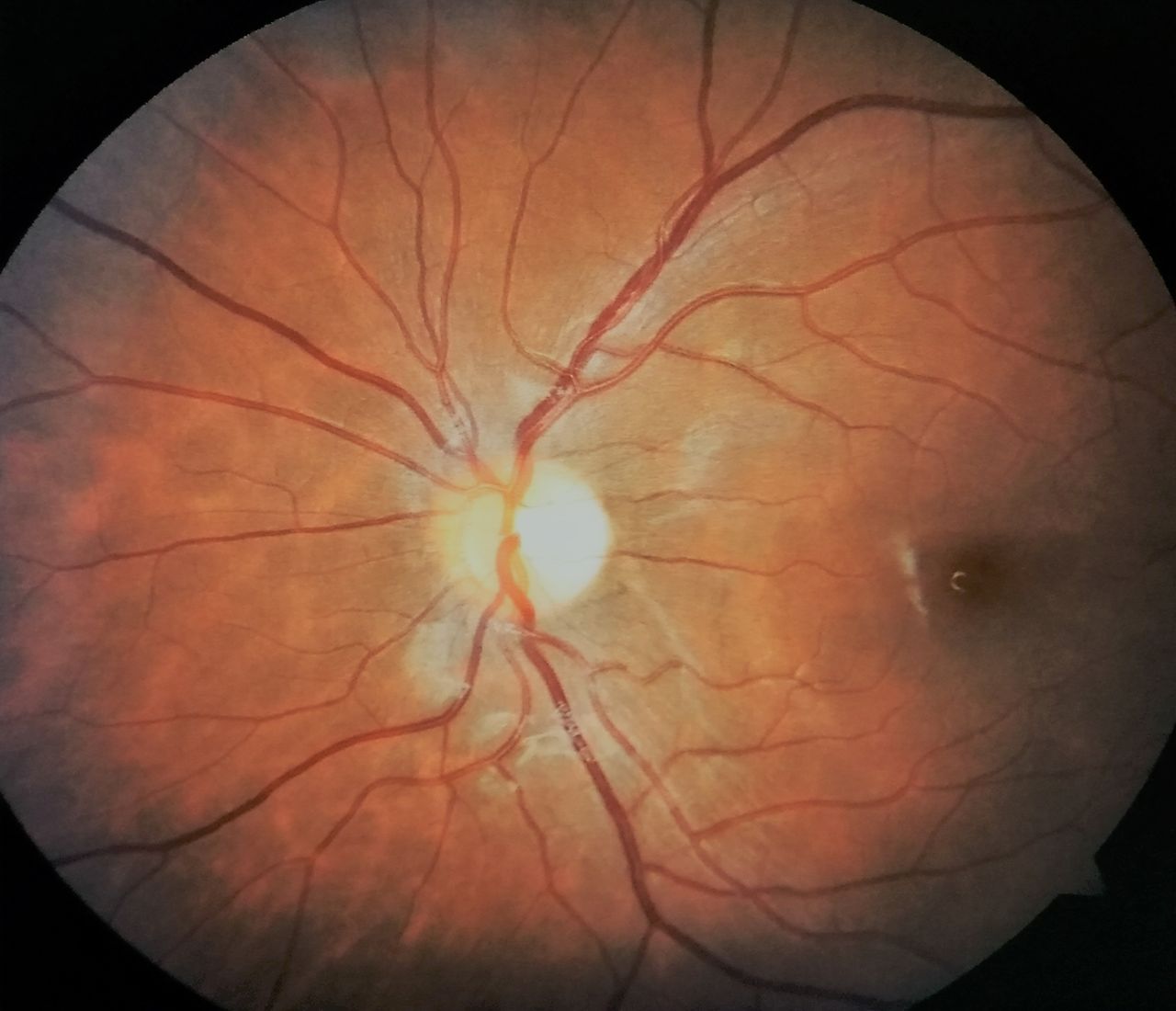
The posterior segment examination, performed after dilation, was essentially normal in the left eye.

{kind=link}
{kind=link}
{kind=link}
The patient underwent cataract extraction surgery with intraocular lens implantation in the left eye. One week after the surgery, the patient’s distance and near visual acuity were recorded to be 20/20 and N6 with +2D, respectively.
The cataracts presenting with petaloid/rosette-shaped opacifications are typically seen in patients who have sustained blunt or penetrating physical trauma to the eye, and rarely due to electric shock, exposure to infrared energy or ionising radiation. The force of the blunt trauma may result in coup, contrecoup injury or axial expansion of the lens.1 The coup ocular injury is a result of direct impact, and results in formation of a Vossius ring as a consequence of compression of the pigmented posterior iris epithelial cells against the anterior lens capsule.2 The contrecoup injury generates shock waves along the line of impact of trauma, and may result in posterior cortical opacification in rosette or stellate shape as seen in our patient.3 The axial expansion causes rapid anterioposterior expansion and may disrupt the lens capsule and/or zonules. These opacifications may appear immediately after, or even up to few months after the trauma is inflicted. The opacities formed due to trauma may be stable or progressive. A thorough ocular examination in such cases is essential to ensure other ocular comorbidities, that is, rupture of globe, subluxation of lenses, choroidal detachment, angle recession glaucoma, retinal detachment, traumatic optic neuropathy, retrobulbar haemorrhage, and so on, are not missed.
Learning points
Atypical stellate/rosette-shaped cataracts may be formed due to exposure to radiation or physical trauma.
High clinical suspicion and a thorough ocular examination are essential to rule out any ocular comorbidity in patients presenting with traumatic cataract.
Footnotes
Contributors RBS and ST authored the manuscript. PI managed the patient, provided the images and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.