Article Text

Statistics from Altmetric.com
Description
A 32-year-old man with a history of symptomatic aortic valve regurgitation was evaluated by our cardiology service. Based on previous clinical investigation and imaging, the patient had been given the diagnosis of bicuspid aortic valve, a diagnosis he carried for well over a decade. As the patient became progressively more symptomatic, a transoesophageal ECG was obtained which demonstrated not a bicuspid, but a trileaflet, thickened valve with an incompetent, deformed right coronary cusp which had severe central regurgitation (figure 1, videos 1–3). The patient underwent mechanical aortic valve repair. Gross anatomical aortic valve evaluation was remarkable for a trileaflet valve with no evidence of fenestrations, endocarditis or perforations. The right coronary cusp had redundant tissue and notable prolapsability, similar to a myxomatous mitral valve. Histopathology of the valve demonstrated disruption of the zona fibrosa layer with expansion of the zona spongiosa. Mucopolysaccharides were deposited within the zona spongiosa consistent with myxomatous changes (figures 2 and 3). A myxomatous heart valve is more classically seen in mitral valve prolapse. However, rarely, myxomatous changes can occur with aortic valves as well and is an under recognised cause of aortic regurgitation. Dilation of the aortic annulus is not a significant factor in the pathogenesis of a myxoid valve and rarely observed on pre-procedural echocardiography. In one case series with over 111 patients, the average age at presentation was 58.1 While historically it was believed that myxomatous valves were secondary to long-standing hypertension, current research favours that hypertension occurs secondary to a chronic regurgitant valve.2 Underlying pathogenesis is incompletely understood but thought to be related to reduction in type I collagen with an ensuing increase in type III collagen. Single enzyme mutations in cardio-specific metalloproteinase protein-2 or alterations in lysyl oxidase enzyme are proposed mechanisms of mitral valve mxyomatous change and prolapse3 4; however, further study regarding the underlying pathology is required before extrapolating this aetiology to mxyomatous aortic valves. Histologically, the valve’s normal collagen-rich fibrosa and spongiosa layer is infiltrated with proteoglycans. Collagen fibres in the myxomatous area have irregular arrangements with poorly formed bundles and the free edge of the aortic valve is often thickened with reactive fibrosis due to regurgitant blood flow. Changes ultimately result in a decrease in cusp stiffness and an increase in extensibility; when coupled with repeated open-and-closure stretching, elongation occurs, further weakening the fibrous core and leading to incompetent valves. In a myxomatous mitral valve, this results in mitral valve prolapse. In this case, worsening aortic regurgitation. The long clinical course from diagnosis to treatment often leads to severe aortic regurgitation with mild to moderate symptoms of heart failure.1 Historically, aortic valve replacement has been the first line treatment. However, aortic valve repair with reconstructive surgery is a possible alternative with fewer periprocedural complications and negates the need for long-term anticoagulation. Reconstructive surgery is customised to the specific cusp defect, typically either a free margin plication or autologous pericardial patch.4 This case is medically significant as it describes a rare aortic valve regurgitation aetiology in a young patient.
Tranthesophageal ECG. Long-axis view with colour Doppler.
Transesophagealc ECG. Short-axis view with colour Doppler.
Transesophageal ECG. Short-axis view.
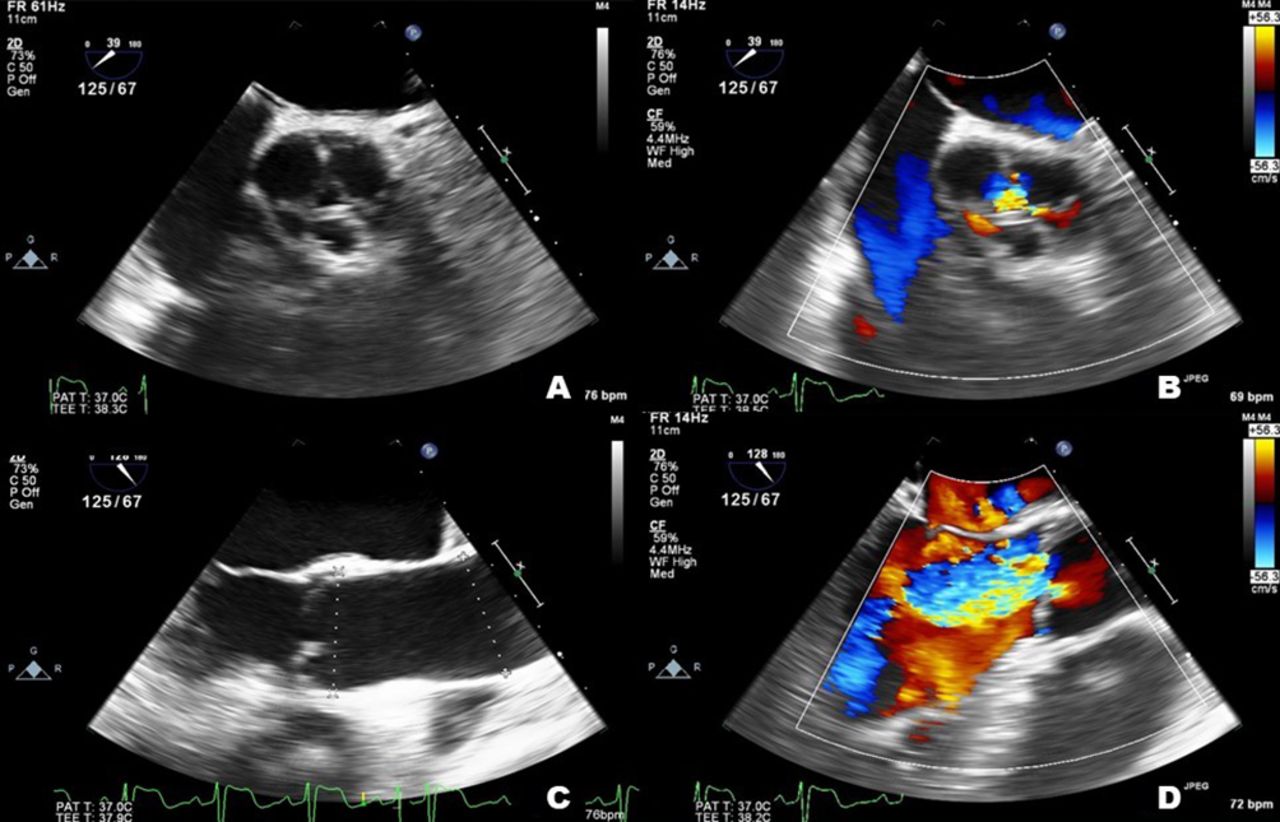
Transesophageal ECG. Short-axis Transesophageal view with and without colour doppler (A, B). Long-axis Tranesophageal view with and without colour doppler (C, D). Aortic root 3.2 cm.

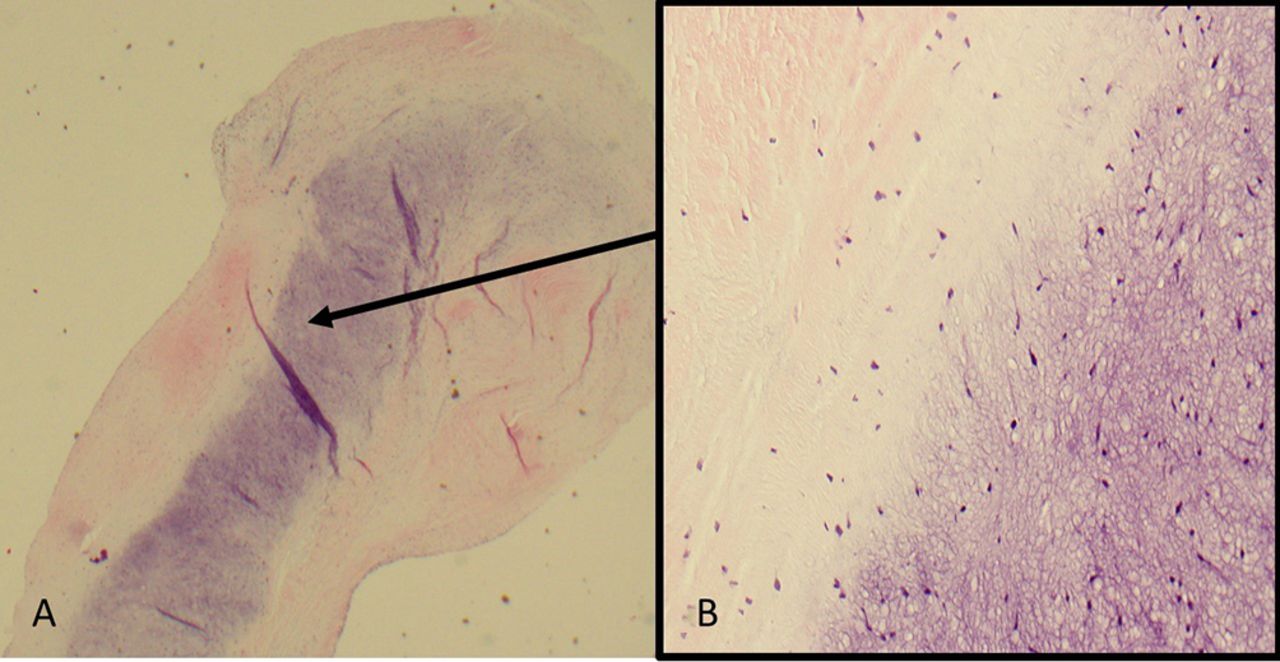
Hematoxylin and eosin stain. Right coronary cusp leaflet: (A) x40 magnification. (B) Selected section x400 magnification. Demonstrating disruption of zona fibrosa layer with expansion of the zona spongiosa. Mucopolysaccharides are deposited within the zona spongiosa.

{kind=link}
{kind=link}
{kind=link}
Movat’s pentachrome stain. Right coronary cusp leaflet: (A) x40 magnification. (B) Selected section x400 magnification. Identifying the disruption of the cusp connective tissue and collagen fragmentation. Mucopolysaccharides are observed in the zona spongiosa.
Patient’s perspective
I remember falling in and out on runs with shortness of breath and for the longest time I could not figure out why. I was so grateful to finally have a reason for my symptoms. Since my surgery my symptoms have improved. While I am no longer in the Army, I am grateful to be able to keep up with my kids as they run around our yard. It was a long process to finally get a diagnosis and treatment, but I am so happy and satisfied with the results. Thank you to all the doctors and nurses involved in my care.
Learning points
Myxomatous aortic valve should be considered in the differential for aortic valve regurgitation especially in patients with structural trileaflet valves in the absence of other abnormalities.
Regurgitation can occur independently of hypertension, endocarditis or connective tissue disease.
Causal aetiology is poorly understood; however, alterations in collagen ultimately result in floppy incompetent cusps and subsequently regurgitant valves.
Footnotes
Contributors CK: data acquisition, manuscript preparation, manuscript draft, and manuscript editing and revision. CM: manuscript preparation and draft editing. DA: manuscript preparation and draft editing. EF: data acquisition, manuscript and draft editing and revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.