Article Text

Summary
An infant, who was born preterm at 36 weeks, presented with fever and ulcer at umbilical region which progressed to necrotising fasciitis of anterior abdominal wall. He was treated with intravenous penicillin, intravenous cloxacillin and local application of medicated honey. Subsequently, he required wound debridement. Postoperatively, he required prolonged invasive ventilation due to poor respiratory effort which was associated with hypotonia and areflexia. Nerve conduction study revealed absent responses. The diagnosis of infant botulism was made based on the clinical presentation, nerve conduction study and his clinical progress. Botulinum immunoglobulin was not available. He was treated with intravenous immunoglobulin and oral pyridostigmine. He was successfully extubated after 37 days, and currently the patient is doing well.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Infantile botulism is a rare neuromuscular disorder resulting from toxins produced by Clostridium botulinum.1 There are seven distinct serotypes named A–G. Only subtypes A, B, E and F cause disease in humans.2 Infant botulism occurs when the clostridial spores of the C. botulinum release botulinum neurotoxin (BoNT) into the bloodstream which irreversibly binds to cholinergic receptors in the presynaptic cell membrane preventing the release of acetylcholine into the synaptic cleft.1
Infantile botulism was first recognised in 1976 in California3 and is most commonly reported in the USA with 128 cases reported to the Center of Disease Control in 2014.4 However, infantile botulism appears to be uncommon in Malaysia. We are not aware of any previous case report.
Case presentation
The infant was born preterm at 36 weeks gestation via spontaneous vertex delivery with birth weight of 2.52 kg to non-consanguineous parents. He was initially admitted and treated with intravenous penicillin and gentamycin for presumed sepsis as he was born prematurely. His initial blood culture was negative, and he was discharged well.
However, at day 10 of life, he was re-admitted for fever and ulcer at the umbilical region. Otherwise, he was active, febrile with a temperature of 38°C and other vital signs were stable with no respiratory distress. He was treated with intravenous penicillin and cloxacillin in addition to local application of medicated honey.
At day 30 of life, his wound condition worsened (figure 1) and he needed wound debridement for necrotising fasciitis of the anterior abdominal wall under general anaesthesia. Postoperatively, he required re-intubation as he was noted to have poor respiratory effort, generalised hypotonia and areflexia.

Picture of the abdominal wound postmedicated honey application and diagnosis of necrotising fasciitis of the anterior abdominal wall was made.
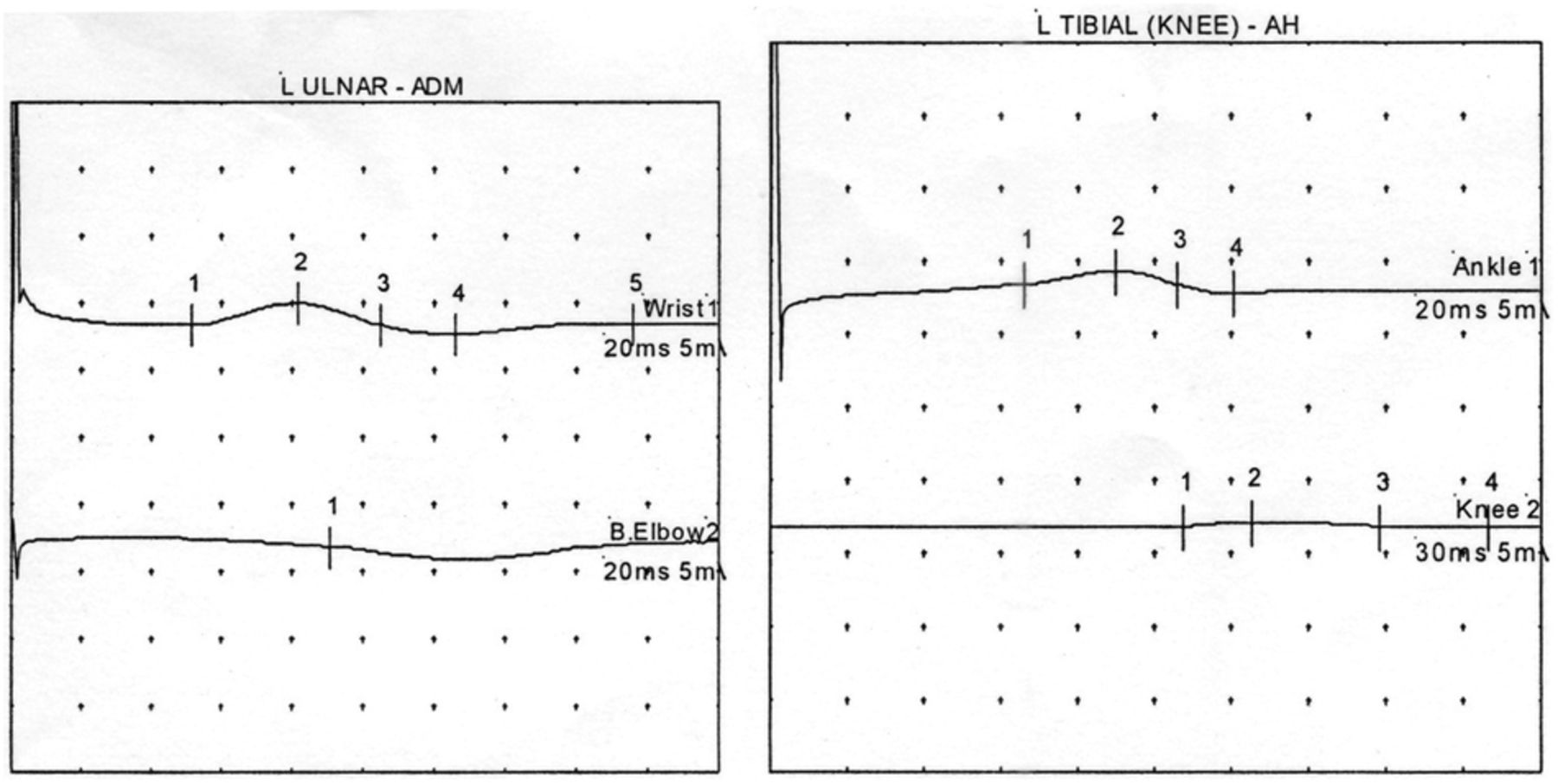
Blood culture was negative, and swab culture showed mixed growth. Nerve conduction study revealed predominantly axonal neuropathy (figure 2). Ultrasound scan of the cranium and lumbar puncture were normal. Primary immunodeficiency screening was negative.

{kind=link}
{kind=link}
Limited nerve conduction study was performed over left ulnar and tibial nerves. The compound motor action potential was reduced with prolonged distal latency. This nerve conduction study was abnormal suggestive of predominantly axonal neuropathy.
The diagnosis of infant botulism was made based on the clinical presentation, nerve conduction study and his clinical progress. He was treated with intravenous immunoglobulin and oral pyridostigmine.
Outcome and follow-up
His condition improved with our supportive care. Subsequently, he was successfully extubated after 37 days and is currently doing well.
Discussion
In infants, botulism may present with constipation, drooling, poor feeding and weak sucking and in extreme cases, loss of muscle tone which may progress to bilateral cranial nerve palsies, flaccid paralysis and diaphragmatic weakness.1 Infants are more susceptible due to the immaturity of the gut flora.1
Honey has been used as a biological wound dressing with broad-spectrum antibacterial activity and high osmolality.5 In this case, the infant presented with infected wound treated with the application of medicated honey raised a high index of suspicion of infantile botulism. There have been case reports associating the ingestion of honey in infants with botulism.6 ,7 ,9
If C. botulinum can be present in ingested honey, it can certainly be present in honey dressings. However, there is no reported case of infant botulism associated with application of medicated honey.
Botulinum toxin is readily detected in stool sample and would confirm the diagnosis. However, this test is currently unavailable in Malaysia.
In 2003, US Food and Drug Administration approved the Orphan Drug Baby BIGR for the treatment of infant botulism which acts by neutralising free botulinum toxin.8 ,10 Treatment should be ideally given as soon as possible after hospital admission and should not be delayed for confirmatory test.
Learning points
This case report highlights the unusual presentation of infant botulism.
To have a high index of suspicion of botulism in an infant who presents with flaccid paralysis in association with a contaminated wound.
Unfamiliarity with the presentation could result in misdiagnosis.
The authors would also like to caution the use of medicated honey for infants.
Acknowledgments
We would like to thank the Director General of Ministry of Health of Malaysia for the permission to publish this case, Associate Professor Dr Lim Kean Ghee MBChB, FRCS, FAMM for critically reviewing this paper, and Dr Goh Pik Pin, Head of Clinical Research Center Malaysia for encouragement and support.
Footnotes
Contributors CJJ, TBK and KYL contributed to conception and design, writing of the abstract and case report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.