Article Text

Statistics from Altmetric.com
Description
The diagnosis and treatment of mesenteric cysts is challenging due to rarity, lack of specific symptoms and variability in location and size. This report aims to discuss current diagnostic and treatment strategies. A 35-year-old woman presented with non-specific abdominal pain. CT revealed a 5×5×3 cm septated abdominal cyst (figure 1). Aspiration (figure 1) demonstrated no malignant cells. Return of symptoms confirmed recurrence using MRI 2 months later (figure 2). Laparotomy confirmed 5 cm cyst attached to ileal mesentery (figure 3). Cyst was excised intact (figure 3). Histology showed multilocular cyst lined by mullerian epithelium. Symptoms resolved with no evidence of recurrence 3 months later (figure 1). Mesenteric cysts, described by Benevenni in 1507, arise from duodenal to sigmoid mesentery. They generally cause non-specific symptoms or rarely rupture, tort and obstruct. They result from lymphatic malformation, occult trauma or infection. Differential diagnosis includes ovarian, duplication or pseudocysts. Careful interpretation of imaging is important for preoperative planning. Ultrasound can be useful as primary imaging modality. Although CT was performed in our case, taking into account the age of the female patient, MRI is advised for further anatomic localisation and guidance for aspiration.1 Treatment is indicated for symptoms. While there is lack of evidence correlating size with complications it is likely that increasing size will increase the risk of complications.2 Complete excision by laparoscopic or open technique is gold standard while simple aspiration or marsupialisation demonstrate higher recurrence rates. While follow-up periods in the literature ranged from 3 to 48 months using ultrasound imaging,3 there appears to be minimal benefits in long-term follow-up as recurrence is rare and generally occurs early.

Axial CT images demonstrating (A) 5×5×3 cm septated cyst (red arrow). (B) CT-guided drainage of cyst. (C). No evidence of recurrence following surgical resection.
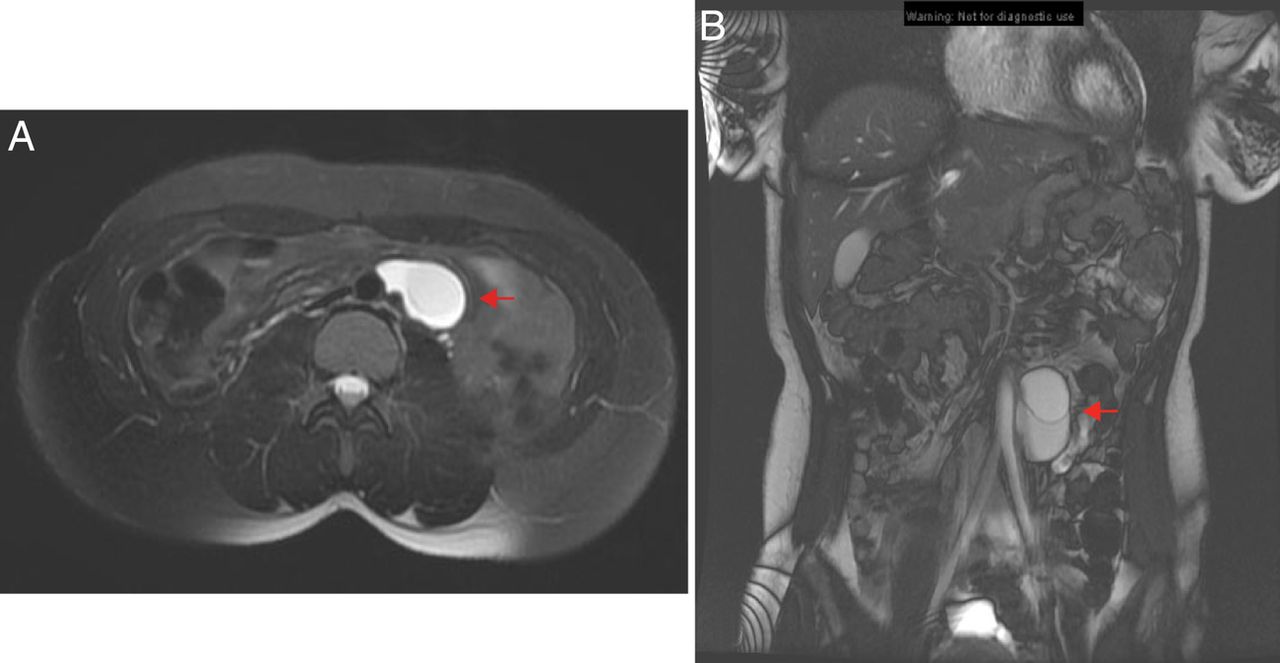
(A) Axial and (B) coronal MRI demonstrating cystic mass in close relation with aorta and extending into ileal mesentery.
{kind=link}
{kind=link}
{kind=link}
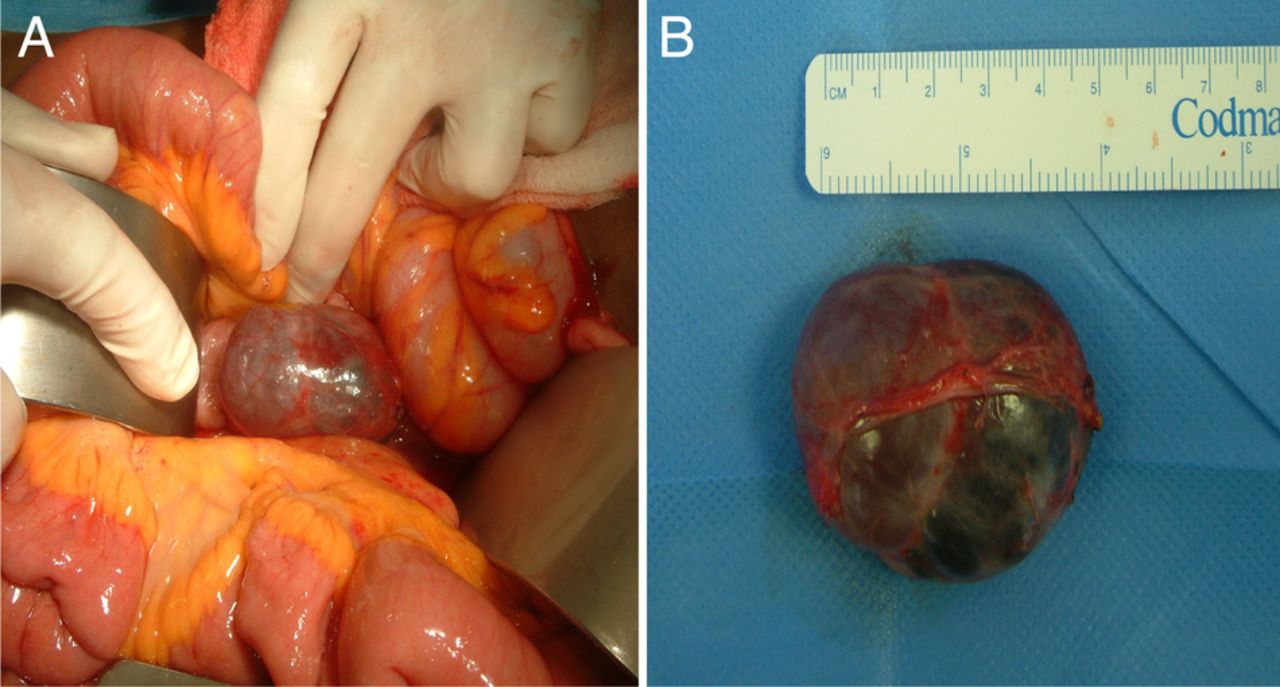
(A) Intraoperative image demonstrating reddish-blue cyst deriving from the mesentery of the small intestine. (B) Completely excised 5 cm mesenteric cyst.
Learning points
-
Mesenteric cysts, a rare cause of abdominal pain, can arise from the mesentery of the duodenum to the sigmoid colon.
-
Preoperative imaging requires careful interpretation for accurate anatomical localisation.
-
Complete excision by either laparoscopic or open technique is the treatment of choice for symptomatic mesenteric cysts.
Acknowledgments
The authors thank South Infirmary Victoria University Hospital.
Footnotes
-
Contributors All the authors have contributed to the management of the patient and drafting the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.