Article Text

Statistics from Altmetric.com
Description
A man in his mid-20s was admitted to the A&E department with melaena and lower abdominal pain. He had been diagnosed with dyspepsia and duodenitis 4 years back.
Haematological investigation revealed microcytic hypochromic anaemia with haemoglobin of 7.7 g/dl and a mean corpuscular volume of 75 fl while other values (including eosinophils) were within normal range. He received blood transfusion and underwent oesophagogastroduodenoscopy (OGD) and colonoscopy which were reported normal. However, routine biopsies taken during OGD showed a mixed inflammatory infiltrate with a high eosinophil count within the lamina propria with no evidence of malignancy.
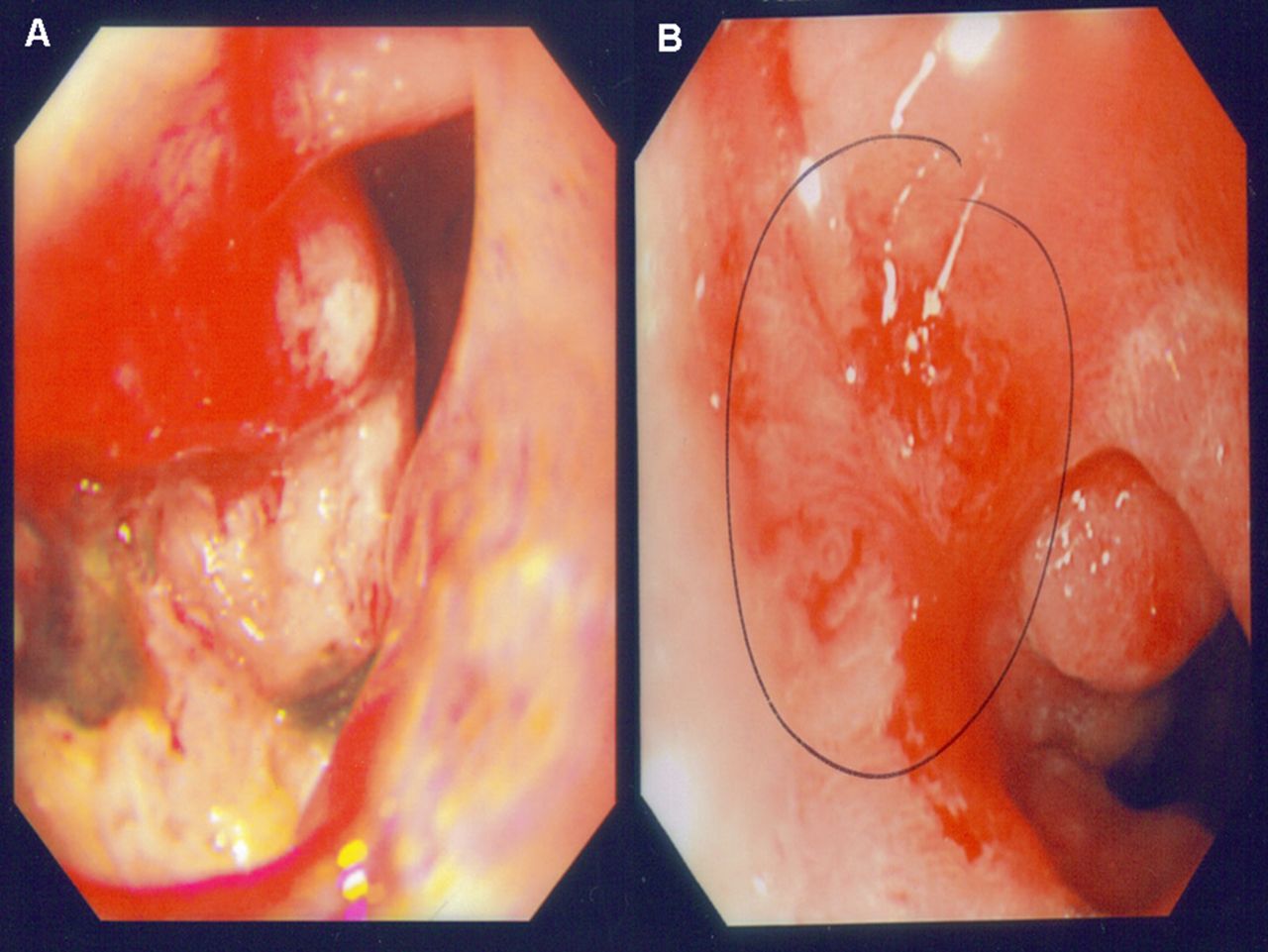
Further investigation with an MRI enterography found evidence of irregular wall thickening and a 4–5 cm stricture with an enhancing irregular wall at D1/D2 with two slightly enlarged regional lymph nodes (figure 1A). To emphasise this, a repeat OGD showed the presence of a large ulcerated mass at the D1–D2 junction (figure 2A). Biopsies taken were consistent with eosinophilic enteritis.
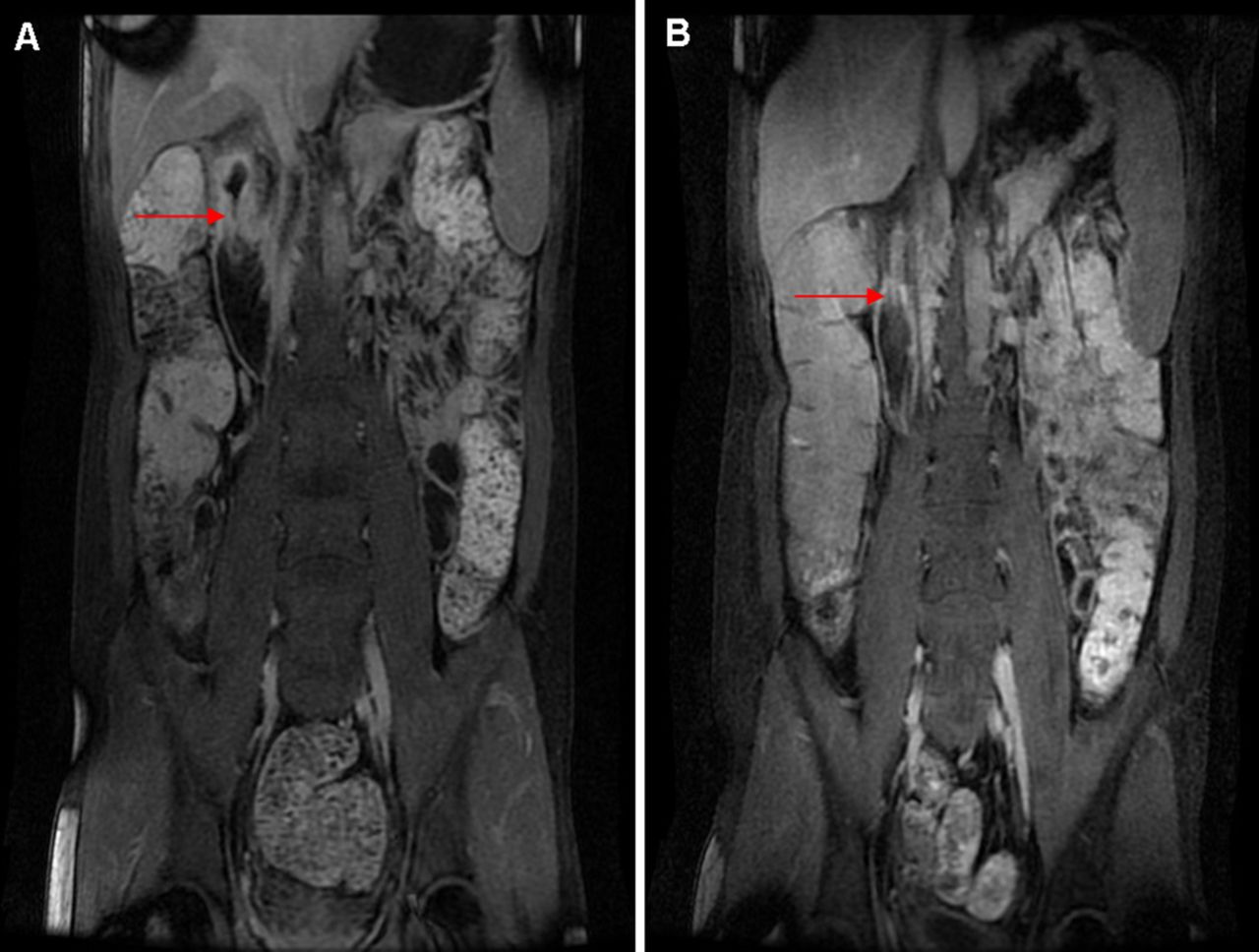
(A) MRI enterography showing irregular wall thickening and 4–5 cm constricting lesion at D1 and (B) showing complete improvement after 16 weeks.

{kind=link}
{kind=link}
(A) Oesophagogastroduodenoscopy shows a large ulcerated mass at D1 and D2 junction and (B) showing healed ulcer with scarring after 10-week steroid treatment.
He was prescribed a 10-week course of reducing regimen of steroids. Following this, he had an OGD which showed a healed ulcer with scarring (figure 2B). Two months later a repeat MRI enterography showed complete resolution in appearance of his D1 and D2 segments with residual small periduodenal lymph nodes (figure 1B).
Learning points
-
MRI enterography is an imaging technique for small bowel disease that is increasingly more popular than CT or barium fluoroscopic examination because of the lack of ionising radiation exposure; improved contrast of the endoluminal, mural and extramural soft tissues.1
-
MRI enterography can also be used to diagnose and monitor activity of inflammatory bowel diseases, identify neoplasms and structural abnormalities.2
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.