Article Text

Summary
An HIV-seropositive man who presented with cough, low-grade fever and difficulty in breathing was admitted to the pulmonology unit at Mulago Hospital in Kampala, Uganda. He was initially diagnosed with bacterial pneumonia and treated with ceftriaxone without significant improvement. Induced sputum and bronchoalveolar lavage specimens were collected and stained using a modified Giemsa stain (Diff-Quik). With this technique, it was possible to demonstrate cystic and trophic forms of Pneumocystis jirovecii and confirm the diagnosis of Pneumocystis pneumonia in this patient.
Statistics from Altmetric.com
BACKGROUND
Pneumocystis jirovecii is an increasingly common but underdiagnosed cause of pneumonia in HIV-infected patients in sub-Saharan Africa. We used a modified Giemsa stain to confirm Pneumocystis pneumonia (PCP) for the first time at Mulago Hospital, in Kampala, Uganda. We believe this report has particular relevance in sub-Saharan Africa, where the burden of HIV/AIDS and opportunistic respiratory infections is high.
In our setting, the diagnosis of PCP is rarely confirmed and we have seen many patients expire while receiving presumptive therapy. This observation is consistent with studies in other settings that have shown that empirical treatment is associated with increased mortality. We believe this case demonstrates the advantages and feasibility of confirming PCP diagnosis using a simple, reliable and affordable technique: the modified Giemsa staining method. More widespread use of this method in low-income countries could help microbiologists and HIV care providers in improving outcomes in HIV-infected patients presenting with pneumonia.
CASE PRESENTATION
An HIV-seropositive man was admitted to the pulmonology unit at Mulago Hospital in Kampala, Uganda, with a productive, irritating cough associated with low-grade fever and progressively increasing shortness of breath of 2 weeks duration. He denied night sweats, chest pain or wheezing. He had been on antiretroviral treatment for 1.5 years, with a starting CD4 T lymphocyte count of 123 cells/μl. He had stopped antiretroviral treatment 7 months prior to admission but remained on co-trimoxazole for PCP prophylaxis. On physical examination, the patient had a heart rate of 112 beats/min, a respiratory rate of 26 breaths/min and an oxygen saturation of 94%. The chest examination demonstrated rales in both lung fields.
INVESTIGATIONS
A chest radiograph showed bilateral, symmetrical, reticular infiltrates in a “bat-wing” distribution. A repeat CD4 T lymphocyte count was not performed on re-admission. Two expectorated sputum samples were submitted on consecutive days for acid-fast bacilli (AFB) smear microscopy and mycobacterial culture, which were negative. Because sputum induction services were not available at Mulago Hospital at the time of hospitalisation, the patient underwent bronchoscopy during which 40 ml of bronchoalveolar lavage (BAL) fluid was obtained. A 10 ml volume was processed for identification of P jirovecii using a modified Giemsa stain (Diff-Quik; Dade Behring, Newark, Delaware, USA) as described below.1
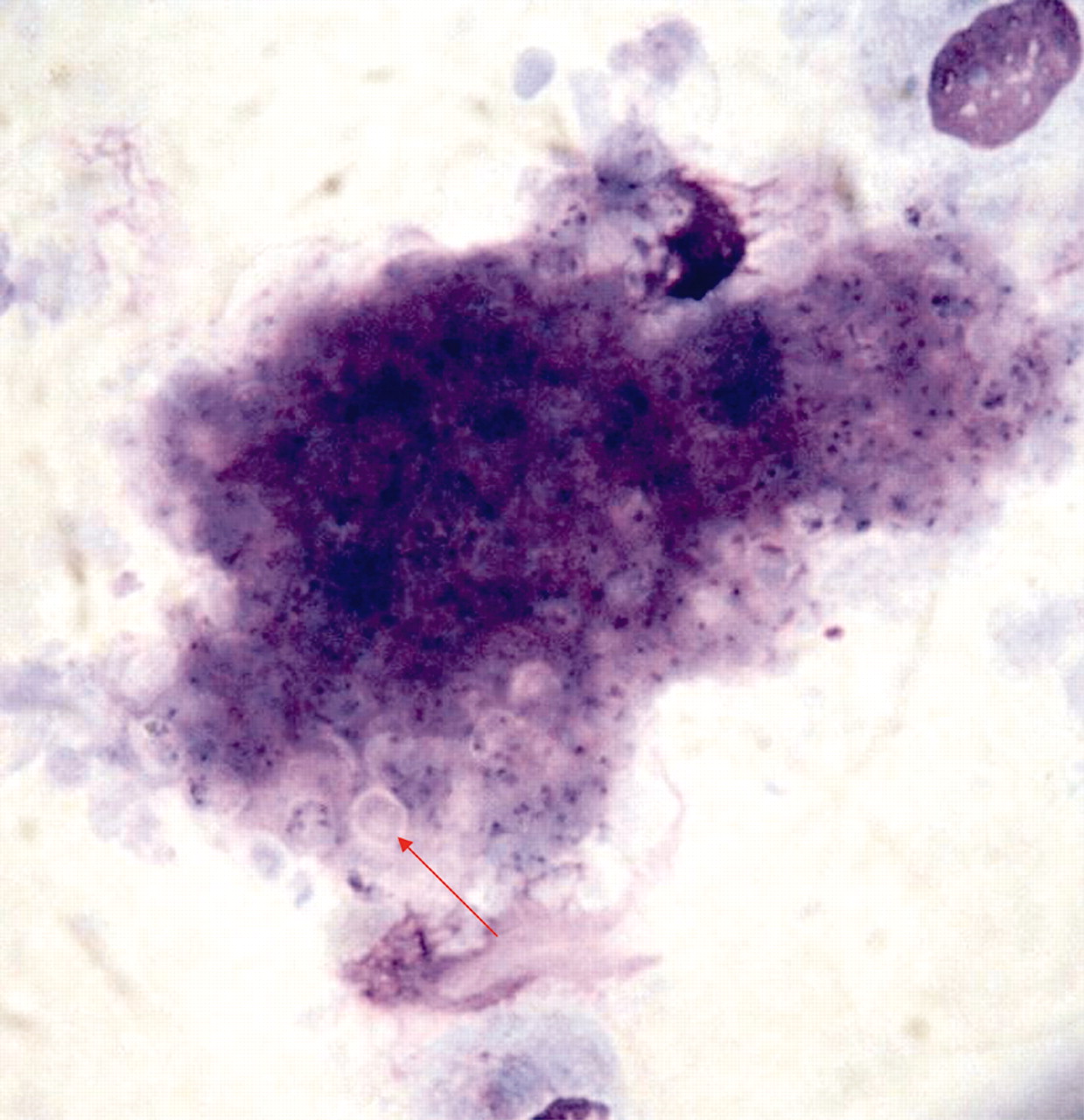
The BAL fluid was centrifuged at 1800 g for 10 min. Smears made from the pellet were air-dried, fixed in acetone for 30 s, and stained using the modified Giemsa method by dipping the slide five times in each of the staining solutions (eosin and Giemsa). Stained slides were examined using a light microscope. A trained microscopist performed the initial search for suspected Pneumocystis organisms using a low-power (×10) objective, and confirmed any abnormalities using a high-power (×100) objective. Using this technique, we were able to demonstrate aggregates of Pneumocystis cysts and discrete trophic forms (fig 1).

{kind=link}
Modified Giemsa stain of bronchoalveolar lavage fluid. Aggregates of Pneumocystis showing round cystic forms with halo-like borders (red arrow) (×1000).
DIFFERENTIAL DIAGNOSIS
The differential diagnosis in this patient with advanced HIV-related immunosuppression included pneumonia caused by community-acquired bacterial pathogens, opportunistic infections (Pneumocystis, Cryptococcus neoformans, Nocardia and mycobacteria), and opportunistic pulmonary malignancies (Kaposi sarcoma and non-Hodgkin lymphoma). HIV-associated inflammatory lung diseases (lymphoid interstitial pneumonia, cryptogenic organising pneumonia) were considered less likely given the radiographic findings.
TREATMENT
Empirical ceftriaxone treatment was started for bacterial pneumonia but resulted in no significant improvement. Following confirmation of PCP, the patient was prescribed high-dose co-trimoxazole with tapering doses of prednisolone.
OUTCOME AND FOLLOW-UP
The patient demonstrated clinical improvement and was discharged from the hospital 5 days after PCP was confirmed, and asked to complete a 21-day course of treatment. He did not return for follow-up.
DISCUSSION
Until now, empirical treatment based on clinical symptoms, physical findings and chest radiography has been the only option for managing suspected PCP cases at Mulago Hospital. Because of resource constraints in sub-Saharan Africa, clinicians do not routinely request laboratory confirmation of PCP, as this may require fibreoptic bronchoscopes, costly immunofluorescence antibody stains, fluorescent microscopes, and trained clinicians and technicians. Despite these difficulties, several published studies have described considerable experience with the use of immunofluorescence antibody staining or PCR assays to confirm PCP diagnoses in research settings in sub-Saharan Africa. The modified Giemsa staining method described here offers a rapid and relatively inexpensive alternative for confirmation of PCP.
Compared with its frequency in HIV-infected patients in high-income countries, PCP was previously thought to be rare in HIV-infected adults in Africa. Early studies (1989–1993) from sub-Saharan Africa reported a PCP incidence among hospitalised patients with pneumonia ranging from zero to 22%.2 Potential reasons for the possible low incidence of PCP in Africa include: (1) inaccurate estimates of the true incidence of PCP because of difficulty in diagnosis; (2) high rates of bacterial pneumonia and tuberculosis in HIV-infected adults in Africa, resulting in death at higher CD4 T-lymphocyte counts and preventing many HIV-infected patients from reaching a stage at which they would be susceptible to PCP; (3) environmental factors, such as seasonal variation; or (4) less virulent regional strains, or lower susceptibility of the African population to PCP. In a study from South Africa, South Africans of European descent had three times the rate of PCP compared with South Africans of African descent.3 Detailed molecular studies of the organism in different parts of the world are needed to resolve these issues.
On the other hand, there is also evidence that PCP might be more prevalent in Africa than previously thought. High proportions of anti-Pneumocystis antibodies among African children suggest that exposure to the organism is common.2 Clinical studies have also documented a higher incidence of PCP among AFB sputum-smear-negative HIV-infected patients – in whom diagnostic testing for PCP is most clearly indicated. Five recent studies in this population have reported a incidence of PCP ranging from 30% to 43%.2 Studies of smear-negative patients with unexplained cough at Mulago Hospital have reported an incidence of PCP of 42% among children and 39% among adults.4,5 These studies affirm the need for inexpensive and feasible methods to confirm PCP diagnosis in HIV-infected patients presenting with pneumonia in our setting.
Several studies have compared the performance of modified Giemsa with other staining techniques used to diagnose PCP. These methods include direct immunofluorescence (DIF), indirect immunofluorescence antibody (IFA), Gomori’s methenamine silver, calcofluor white, and modified toluidine blue-O stains. Compared with these other techniques, modified Giemsa has similar diagnostic accuracy, and is faster and easier to perform.6 The sensitivity of modified Giemsa ranges from 58% to 92% in induced sputum, and from 81% to 100% in BAL fluid; the specificity is greater than 97% in both specimen types.6,7 These performance characteristics compare favourably with those of other techniques.6,7 At a cost of US$1.50 per test, modified Giemsa is inexpensive compared with the DIF and IFA tests,7 and the stability of the stain at room temperature allows easy storage. Finally, the modified Giemsa technique stains respiratory epithelial cells for cytology, as well as other common opportunistic respiratory pathogens, including Toxoplasma gondii, Cryptococcus neoformans, Histoplasma capsulatum and cytomegalovirus. All of these features make modified Giemsa an ideal multipurpose stain for diagnosis of respiratory pathology in HIV-infected patients in low-income countries.
LEARNING POINTS
-
Modified Giemsa is a highly sensitive, simple, accessible and inexpensive procedure that requires only basic laboratory equipment.
-
Previous studies have shown that microbiological confirmation of Pneumocystis pneumonia diagnosis is associated with decreased mortality compared with empirical treatment.
-
Adoption of the modified Giemsa technique in low-income countries may improve outcomes in HIV-infected patients presenting with pneumonia.
Acknowledgments
This work was supported by grants K24HLO87713 and F32HL088990 from the National Heart Lung and Blood Institute at the National Institutes of Health. The authors would like to acknowledge Barbara Haller, Carol Goodman and Karen Gleason from the Department of Microbiology at San Francisco General Hospital for teaching the Diff-Quik technique to laboratory technicians at Mulago Hospital.
Footnotes
Competing interests: none.