Article Text

Statistics from Altmetric.com
DESCRIPTION
The non-recurrent inferior laryngeal nerve (NIRLN) is a rare anomaly (0.5–0.6% on the right side, extremely rare on the left side (0.004%)), which increases the risk of damage to the nerve during surgery. The right NRILN is associated with a right subclavian artery arising directly from the aortic arch. The left NRILN is associated with situs inversus.1–3
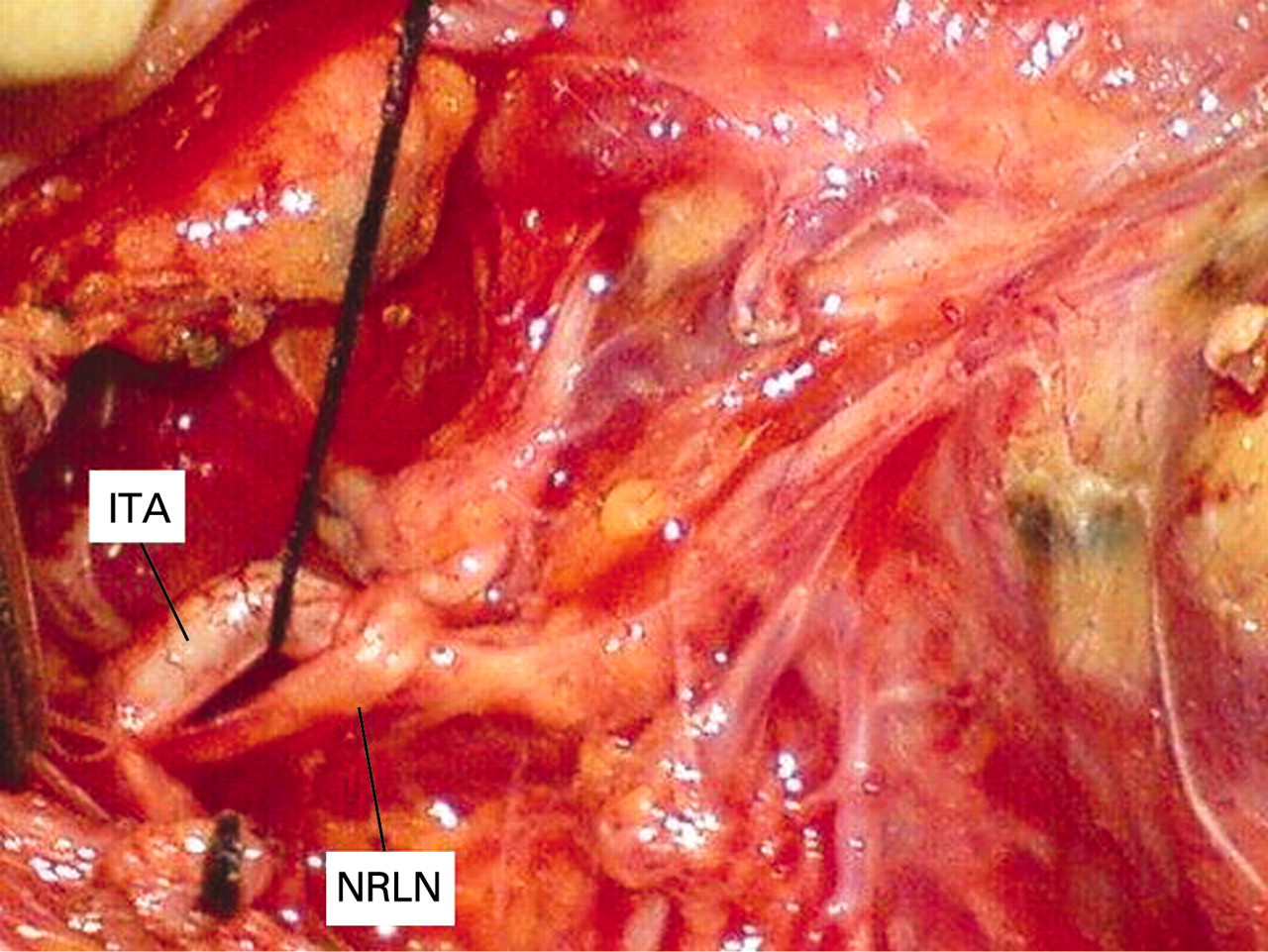
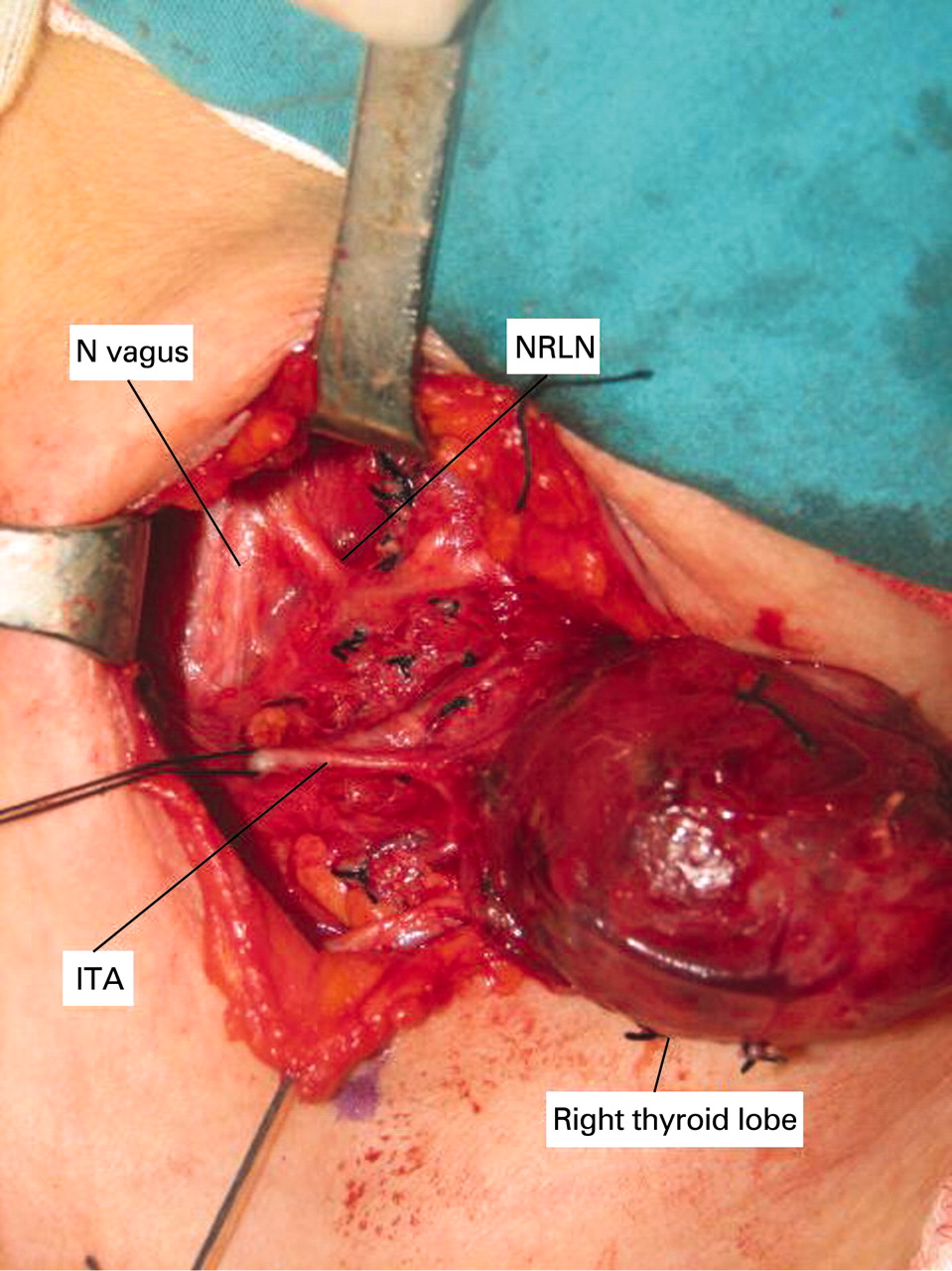
The origin of the NRILN is cervical. Three types can be distinguished: type 1 NRILN arises directly from the vagus and runs together with the vessels of the superior thyroid pedicule; type 2A (fig 1) NRILN follows a transverse path parallel to and over the trunk of the inferior thyroid artery; and type 2B (fig 2) NRILN follows a transverse path parallel to and under the trunk or between the branches of the inferior thyroid artery.2

Right lateral view from a patient with non-recurrent laryngeal nerve (NRLN) undergoing thyroidectomy toxic multinodular goitre. The NRLN arises directly from the cervical part of the nerve (N) vagus and follows a transverse path parallel to and over the trunk of the inferior thyroid artery (ITA). The NRLN is divided into the two branches before passing to the ligament of Berry.
{kind=link}
{kind=link}
Right lateral view from a patient with non-recurrent laryngeal nerve (NRLN) undergoing thyroidectomy for recurrent goitre. The NRLN arises directly from the cervical vagus and follows a transverse path parallel to and under the trunk of the inferior thyroid artery (ITA).
During thyroid and parathyroid surgery, the best way to avoid morbidity is to identify the nerve on both sides with a systematic dissection based on usual anatomic landmarks. When the inferior laryngeal nerve is not found in a classic position, the presence of a non-recurrent nerve is suspected. Any transverse bond should not be cut between the carotid artery and larynx except the middle thyroid vein. If the presence of the non-recurrent nerve is unknown, nerve injury can easily occur during surgery. Therefore, awareness of their existence and anatomic variations and correct surgical technique will prevent the surgeon from accidentally damaging the NRILN.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.