Article Text

Abstract
Entamoeba histolytica is a cosmopolitan pathogenic parasite. It is spread via the feco-oral route and, to a lesser extent, via sexual intercourse. We report a case of hepatic and intestinal amoebiasis in a 67-year-old man who had never travelled to an endemic area. Abdominal CT investigations detected two liver abscesses and chronic colitis. Positive amoebic serology and a positive PCR test for E. histolytica in the hepatic liquid and faeces confirmed the diagnosis. Curative metronidazole and tiliquinol-tilbroquinol were administered successfully. The patient had been contaminated through heterosexual intercourse with his healthy French female partner who was a carrier of the parasite. Though unusual, amoebiasis as a result of sexual transmission should be considered in non-endemic areas in people who have never travelled abroad, particularly in the presence of clinical symptoms such as liver abscesses or chronic diarrhoea.
- tropical medicine (infectious disease)
- liver disease
- sexual transmitted infections (bacterial)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Entamoeba histolytica is a protozoan that causes non-febrile intestinal infection or febrile hepatic infection, and it is the third most deadly parasitic infection. Amoebiasis is highly prevalent in low-income and middle-income countries and is mainly transmitted via the feco-oral route.1 In high-income countries, amoebiasis usually occurs in migrants and travellers returning from endemic areas. To a lesser extent, it can be also transmitted sexually, in particular with men who have sex with men.2 Genuine European autochthonous cases are scarce.3–6 We present here a rare case of a French heterosexually contracted autochthonous amoebiasis.
Case presentation
In July 2018, a 67-year-old French man was admitted to hospital for liver pain associated with fever. He was on irbesartan 300 mg per day for chronic hypertension. He was retired from the public service and had a female partner. He had never travelled outside Europe.
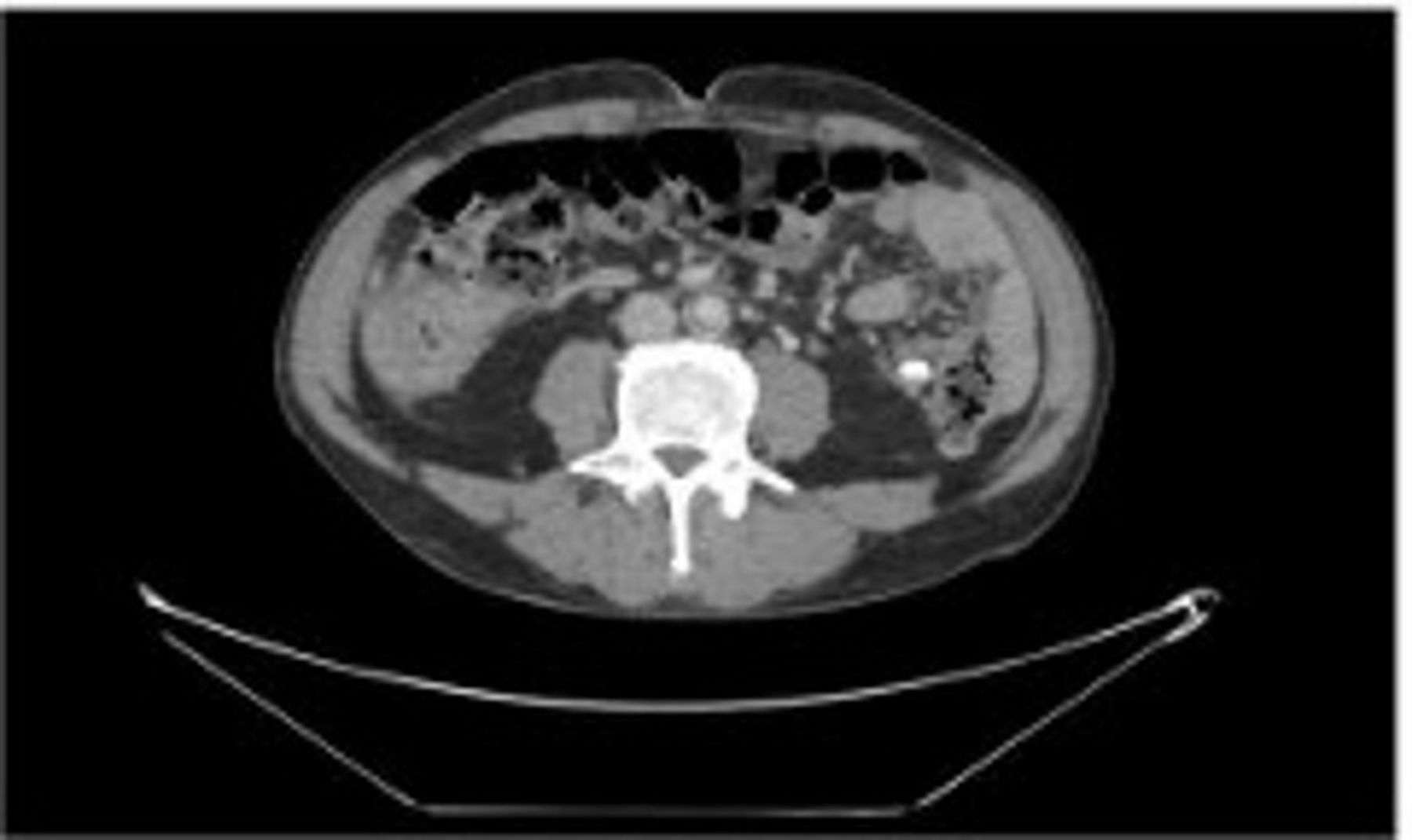
Six months previously, he had developed non-febrile bloody diarrhoea (5–15 stools per day). He consulted his general practitioner only 3 months after the start of symptoms. The bacterial stool culture was negative at this time. Ciprofloxacin 500 mg two times per day for 7 days was not effective. Three months later, he presented to the emergency room for right upper quadrant pain, associated with fever for the past 48 hours. He had a low-grade fever (38.5°C), blood pressure was 120/60 mm Hg and his pulse was 110 bpm and regular. He reported losing 5 kg over the past 6 months. His right upper abdominal quadrant was hypersensitive, but there was no clinical hepatomegaly or jaundice. No other abnormality was detected. His blood results were as follows: haemoglobin 117 g/L, white blood cells 20×109/L (mainly neutrophils), C reactive protein 298 mg/L, total bilirubin 10 µmol/L, serum creatinine 90 mmol/L, alanine transaminase (ALT) 38 IU/L, aspartate transaminase (AST) 23 IU/L and serum albumin 19 g/L. He tested negative for HIV, and there was no hypogammaglobulinaemia. Abdominal and pelvic CT showed two hepatic abscesses in the VI and VII segments (58 and 67 mm in diameter, respectively) (figure 1) and signs of chronic colitis and proctitis (figures 2 and 3).

Abdominal CT showing the two cystic abscess cavities.

Abdominal CT showing chronic colitis.

{kind=link}
{kind=link}
{kind=link}
Abdominal CT showing simultaneous intestinal and hepatic amoebiasis.
Investigations
A reddish fluid was aspirated from the hepatic abscesses with the use of ultrasonography (US) guidance. Blood cultures were sterile. The bacterial stool culture was negative. The faeces were negative for Clostridium difficile and Cryptosporidium. In the fluid taken from the liver abscess, bacterial and mycobacterial cultures were negative, but PCR for E. histolytica was positive. E. histolytica was also positive in the faeces. Amoebic serology was positive with a titre superior to 1/2560 (cut-off >1/320), confirming a diagnosis of autochthonous intestinal and hepatic amoebiasis.
Differential diagnosis
In the case of our patient, three diagnoses were possible (in order of probability):
1. A bacterial abscess from a digestive tract infection.
2. A bacterial abscess secondary to infectious endocarditis.
3. A parasitic abscess.
Treatment
After percutaneous drainage, the patient started on intravenous ceftriaxone 2 g per day and metronidazole 500 mg three times per day. Ceftriaxone was stopped after 3 days once the amoebic serology was known to be positive. Overall, the patient was treated with metronidazole for 10 days followed by tiliquinol-tilbroquinol two tablets two times per day for 10 days.
Outcome and follow-up
Within 48 hours, fever, bloody diarrhoea and hepatic pain disappeared, and most of his laboratory parameters normalised. At follow-up 2 months later, no recurrence was observed and the stool sample was negative.
Way of transmission
The patient had never travelled outside of Europe, but his French female partner had travelled in endemic areas including South America, India, Burma, Vietnam and Laos. She had also had a prior heterosexual relationship with a man who was diagnosed with intestinal amoebiasis. She had never presented symptoms. Her serology was positive with a titre superior to 1/2560, but abdominal US did not show liver abscess. She was started on metronidazole 500 mg three times daily for 10 days followed by tiliquinol-tilbroquinol two tablets twice daily for 10 days. At follow-up 2 months later, E. histolytica serology was negative.
Discussion
Though European cases are quite rare, E. histolytica protozoan is cosmopolitan and autochthonous cases may occur in metropolitan France.3–5 A diagnosis of E. histolytica should not be ruled out only because the patient has not visited travel in endemic areas. Though it is transmitted via the feco-oral route, it may also be to a lesser extent sexually transmitted from healthy carriers. Additional risk factors for amoebiasis infection have been identified, such as men having sexual relationship with men,2 HIV coinfection7 or oro-anal sexual practices,8 but our patient confirmed having an exclusively heterosexual relationship with his female partner.9 Very few heterosexually transmitted cases have been reported, but three cases of hepatic abscesses were reported in a group of Canadian tourists who had intergroup sexual relationships.8 More recently in France, a case of amoebiasis was reported in a male with no risk factor apart from a sexual relationship with a South African woman.5
Our patient presented simultaneous intestinal and liver amoebiasis. Classically, intestinal mucosa invasion leads to an intestinal infection, which then develops into ulcerations and microabscesses, resulting in non-febrile (bloody) diarrhoeas. Then, the liver may be infected by invasion of the portal venous system. Hepatic tissue necrosis creates hepatitis abscesses resulting in pain and fever.1 To our knowledge, there are very few cases of simultaneous intestinal and hepatic clinical forms in the literature.9 10 Hepatic abscesses are more prevalent in males and are associated with gastrointestinal symptoms in 10%–35% of patients.1
Intestinal amoebiasis is usually confirmed with a parasitic stool culture, a PCR-based test or presence of E. histolytica on colonic mucosal biopsy specimens. Hepatic amoebiasis can be confirmed with serology (gold standard), but its positivity may be sometimes delayed. Most of time aspiration of the abscess is required to rule out a pyogenic abscess. Occasionally, the abscess may require drainage in patients who fail to respond to drug therapy with a high risk of abscess rupture (cavity with a diameter of more than 5 cm) or for pain relief.1
Treatment for intestinal or hepatic amoebiasis consists of a sequence of two antiparasitic therapies. First, a nitroimidazole drug is prescribed, specifically metronidazole (500 mg three times per day for 10 days), followed by a luminal infection cure such as tiliquinol-tilbroquinol (two tablets two times per day for 10 days) or diloxanide furoate. Treatment of the luminal infection is needed to avoid a relapse. Clinical follow-up is associated with a stool culture 3–4 weeks after the end of treatment.2 As amoebiasis can be transmitted via sexual route, it is essential to identify and treat sexual partners to avoid recontamination. This is important in developed countries like France where, though recent epidemiological data are lacking, it has been suggested that 11% of sewer workers and 2% of the general population carries Entamoeba dispar/E. histolytica.11 There are also increasing numbers of migrants12 and travellers from endemic areas who are potential carriers of E. histolytica, as shown in our case. The recommended treatment for a healthy carrier is the luminal infection cure also1; invasive infection therapy like metronidazole is not required.
Learning points
This is an original and rare case of French autochthonous amoebiasis transmitted by a heterosexual French partner.
Simultaneous intestinal and hepatic amoebiasis is a rare but possible diagnosis.
This case illustrates the interest of testing for Entamoeba histolytica in patients with chronic diarrhoea or hepatic abscess, even if the patient did not travel to an endemic area.
It is important to consider the possibility of heterosexual transmission and to screen and treat sexual partners to avoid recontamination.
For individuals who have travelled to endemic areas, amoebiasis could be considered in addition to syphilis, HIV, hepatitis B and C when screening for sexually transmitted infections. This could be an efficient way to identify healthy carriers and limit the spread of amoebiasis.
Acknowledgments
The authors thank Mrs Rankin Suzanne for the English grammar revision.
Footnotes
Contributors ACB carried out the literature search of sexual transmitted infection by Entamoeba histolytica cases and collected all the data so far published. She then worked with CM in writing down the paper. ASR and LP have read and helped in completing the final manuscript. LP was involved in the initial diagnosis and management of the patient and helped in completing the final manuscript. CM was involved in the management and follow-up of the patient and helped in writing and completing the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained