Article Text

Abstract
Diffuse intestinal ganglioneuromatosis is a rare condition associated with MEN2B. It is also seen in conditions like neurofibromatosis type 1 and Cowden syndrome. This is a report of a patient who underwent total colectomy with end ileostomy creation for a megacolon. He was diagnosed to have diffuse ganglioneuromatosis on histological examination of the resected segment of colon. The definitive management of diffuse ganglioneuromatosis is to resect and anastomose.
- thyroid disease
- gastrointestinal surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Multiple endocrine neoplasia (MEN) is a clinical entity associated with multiple endocrine tumours.1 Tumours range from benign to malignant. MEN can be either type 1 or type 2.
Type 2 is further classified into types 2A and 2B. Type 2A is associated with tumours arising from thyroid, parathyroid and adrenal gland, whereas type 2B has tumours arising from the thyroid and adrenal gland. Type 2B is associated with phenotypic changes like marfanoid body habitus and multiple mucosal neuromas in the eyes and lips. Other causes of marfanoid body habitus include Shprintzen-Goldberg syndrome, Ehlers-Danlos syndrome and Homocystinuria.2
Eighty per cent of medullary thyroid cancer occur sporadically and approximately 20% are inherited with RET (rearranged during transfection) mutation.3 MEN2B is associated with a much more virulent form of medullary thyroid cancer than 2A. MEN2B is associated with RET proto-oncogene mutation.
Diffuse ganglioneuromatosis is a hamartomatous polyposis condition characterised by mural or transmural proliferation of neural elements in the enteric plexuses. It is seen in conditions like neurofibromatosis-1 (NF-1), MEN2B and Cowden syndrome.4 The diagnosis of diffuse ganglioneuromatosis is confirmed by histology. These patients commonly present with altered bowel habits or gastrointestinal bleeding or both.
Case presentation
A 36-year-old man who was diagnosed to have MEN2B presented with worsening constipation and abdominal distension of 3 months duration. He was diagnosed to have MEN2B while being evaluated for disseminated medullary thyroid cancer at the age of 18 years. The metastatic deposits of medullary thyroid cancer were found, when the patient was evaluated for right side painful inguinal lymphadenopathy.
The patient had clinically significant constipation for 3 months. Despite having constipation for 3 months, due to socioeconomic constraints, the patient only presented when he developed absolute constipation with worsening abdominal distension. He had no other features of bowel obstruction including associated vomiting or abdominal pain.
Even though he required thyroxine replacement following total thyroidectomy for medullary thyroid cancer, he had poor compliance to treatment. The patient also had a neuropathic bladder and was on an indwelling urinary catheter since childhood.
On general examination, the patient was ill looking and in discomfort. He was afebrile. Patient had peripheral pitting oedema. He had marfanoid features including arachnodactyly, high arched palate and pectus excavatum. Mucosal neuromas were seen in the eyelids, lips and tongue (figure 1). On examination of the abdomen, it was grossly distended without features of peritonism. There was flank dullness on percussion and sluggish bowel sounds on auscultation. Digital rectal examination revealed an empty rectum. He was haemodynamically stable.

Mucosal neuromas.
Investigations
Initial blood investigations showed a white cell count of 9.6x 109/L/ and a haemoglobin concentration of 102g/L. His serum creatinine was normal. His serum albumin was low at 22 g/L and the thyroid stimulating hormone level was 150 mIU/L due to poor compliance to thyroxine replacement. The X-ray abdomen showed a grossly dilated large bowel with a maximum diameter of 7 cm. Caecum was dilated to 12 cm. The rectal gas shadows were absent.
Differential diagnosis
Colonic tumour.
Colonic stricture.
Foreign body obstruction.
Treatment
A laparotomy was performed for megacolon with absolute constipation. During the laparotomy, large bowel was grossly dilated with sparing of the rectum and small bowel (figure 2). There were no ischaemic segments. Colon was mobilised from right side proceeding to the left side with hepatic flexure and splenic flexure mobilisation. Total colectomy was done (figures 3 and 4) and an end ileostomy was created.

Intraoperative findings of megacolon.

Resected total colectomy specimen.

Cut surface of the resected specimen with impacted faecal material.
Outcome and follow-up
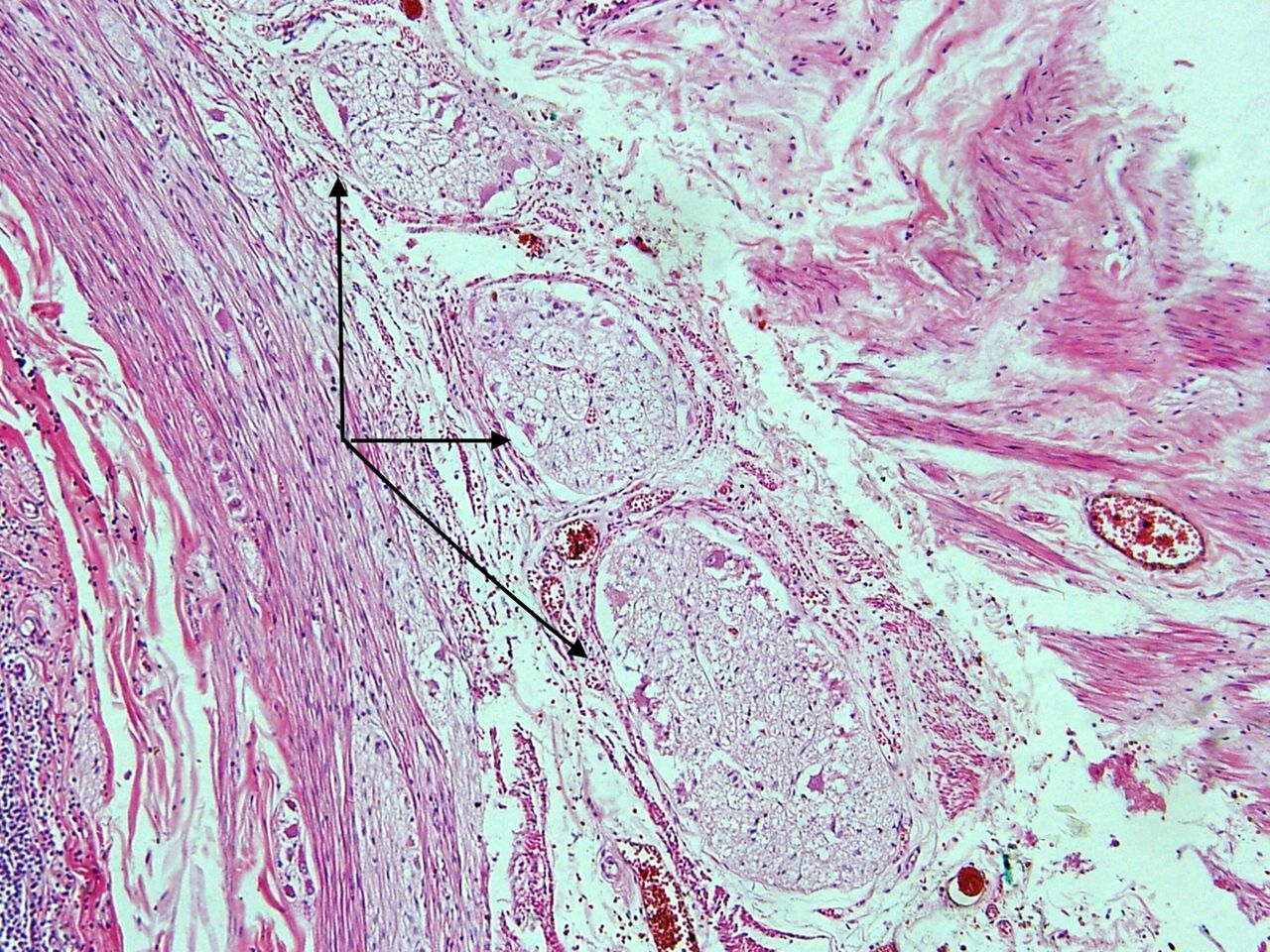
He had an uncomplicated postoperative period. The patient was discharged and was followed up in the surgical clinic. Histopathological evaluation of the resected specimen showed ‘diffuse ganglioneuromatosis of the colon’ (figures 5 and 6).

Histological specimen of patient showing hypertrophied nerve bundles (arrow heads)in the myenteric plexus.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Magnified view of the hypertrophied nerve bundles in the myenteric plexus (arrow heads).
Discussion
MEN can be of two types. Type 1 is associated with tumours arising from the pituitary gland, parathyroid and pancreas. Type 2 has 2A and 2B varieties. MEN2B has several eponyms including Williams-Pollock syndrome, Gorlin-Vickers syndrome and Wagenmann-Froboese syndrome.
MEN type two is associated with RET mutation. The RET mutation can give rise to MEN2A, 2B or familial medullary thyroid cancer. Therefore, clinical entity that manifests via RET mutation depends on the codons and exon that is affected in the RET gene.3
Medullary thyroid cancer is almost always present in MEN2B.1 Prophylactic thyroidectomy is recommended in patients carrying the RET mutation under the age of 5 years.3 MEN2B is associated with a virulent form of medullary thyroid cancer with early dissemination to lymph nodes and early thyroidectomy is warranted. Our patient had disseminated medullary thyroid cancer when it was diagnosed at 18 years, with a positive inguinal lymph nodes. He underwent total thyroidectomy with lymph node block dissection followed by chemotherapy. Surgery with total thyroidectomy is the main mode of management despite metastatic disease.5
Intestinal ganglioneuromas are rare benign tumours. It can occur as a localised pathology with a single polypoidal ganglioneuroma or as multiple polyps. Laudari et al described a case report of an isolated ganglioneuroma of the descending colon in a patient who had no associated features of MEN2B or NF-1.6 In diffuse ganglioneuromatosis, multiple neuroma can occur in the myenteric and submucosal plexuses. Macroscopically, it manifests as gut wall thickening.7 This condition is associated with NF-1, Cowden syndrome and MEN2B syndrome. In MEN2B, myenteric plexus is more involved, whereas submucosal plexus is more involved in NF1. In diffuse ganglioneuromatosis, the entire colon may be involved with sparing of the small bowel.8
Diffuse ganglioneuromatosis can present with per rectal bleeding and altered bowel habits such as constipation. Diffuse ganglioneuromatosis can even present with megacolon as seen in this case report and few other reported cases.9 This condition responds poorly to medical management and therefore, best managed with surgical resection.7 As this condition is very rare, it is usually not included in the differential diagnosis of pseudo-obstruction. The diagnosis of diffuse ganglioneuromatosis is confirmed by histology,7 which shows proliferation of nerve cells in the enteric plexuses. In most case reports, diffuse ganglioneuromatosis with MEN2B presents early in childhood with pseudo Hirschsprungs features, even prior to manifestation of medullary thyroid cancer.4
Gfroerer et al describe constipation (72%) as the most common gastrointestinal symptom in patients with MEN2B. He evaluated 55 patients with MEN2B in published literature and showed that more than 50% of patients presented with constipation below the age of 1 year.10
Huston et al described a case report where a 1-month baby who presented with constipation and was diagnosed with MEN2B following a rectal biopsy. The baby subsequently underwent a thyroidectomy at 9 months and a colectomy at 4 years.11 The presence of ganglions among enlarged nerve fibres distinguishes Hirschsprungs from MEN2B.12 Gibsons et al described 8 cases of megacolon out of 11 cases with MEN2B using the Mayo Clinic Registry over a period of 20 years. All of the reported cases with megacolon presented with constipation in early childhood or infancy.9
However, the unique presentation of our patient is that he presented late with troublesome constipation and megacolon at the age of 36 years. This presentation was even after being treated for disseminated medullary cancer at the age of 18 years at a tertiary care hospital. Our patient suffered from less than three bowel motions per week, straining during 25% of defecatory time, passing hard stools and also digitation to empty the rectum. These symptoms satisfy ROME IV criteria in the diagnosis of constipation which requires further evaluation. Despite having significant constipation for 3 months, the patient did not seek medical attention as he was from a rural area in Sri Lanka with limited access to tertiary healthcare facilities.
His clinically subtle constipation may have worsened by overt hypothyroidism caused by poor compliance to thyroxine. Therefore, a patient with MEN2B syndrome presenting with constipation, diffuse ganglioneuromatosis should be entertained in the differential diagnosis even in adults.
Learning points
In most case reports, diffuse ganglioneuromatosis with MEN2B presents early in childhood with pseudo Hirschsprungs, even prior to manifestation of medullary thyroid cancer.
Therefore, even among adults with multiple endocrine neoplasia syndrome presenting with constipation, diffuse ganglioneuromatosis should be considered in the differential diagnosis.
The diagnosis of diffuse ganglioneuromatosis is confirmed by histology.
Acknowledgments
We would like to acknowledge the support rendered to us by Professor N R Perera and Dr L J De Silva of the Histopathology Department of Faculty of Medicine University of Colombo.
Footnotes
Contributors All authors contributed to the care of the patient. Dr ARF wrote the initial draft of the manuscript and Professor DNS and Dr RPB contributed with modifying the overall content in manuscript. All authors read and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.