Article Text

Abstract
Rhabdomyolysis is characterised by muscle breakdown with release of damaging proteins that can have devastating consequences. Acute influenza infection is being increasingly recognised as an underlying aetiology. We report an unusual case of severe rhabdomyolysis with acute renal failure due to influenza A infection that improved with high-dose oseltamivir and intravenous fluids. In our case, we also noticed a temporal relation between fever spikes and subsequent increase in serum creatine kinase. The precise mechanism between the rise in temperature and creatine kinase is unclear but it could be due to direct viral invasion of myocytes or due to release of new viral progeny following replication in the myocyte.
- drugs: infectious diseases
- influenza
- adult intensive care
- acute renal failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Influenza A infection is most commonly associated with pulmonary disease ranging from a mild upper respiratory tract infection to severe pneumonia. However, other important manifestations include myocardial infarction, Guillain-Barré syndrome, encephalitis, pericarditis and rarely severe rhabdomyolysis. While myalgias are a common complaint in patients with acute influenza infection, acute myositis and rhabdomyolysis are likely under-reported.1 Even though rhabdomyolysis occurs more frequently in children, it is now increasingly recognised in adults. In one series, 62.5% of patients (n=18, median age 38 years) with influenza A had elevated creatine kinase (CK) above 200 U/L on admission (range 58–2156 U/L).2 Current influenza guidelines do not address CK measurement. Previous studies and our case suggest CK measurement be part of the workup for the hospitalised patient with acute influenza infection.
Case presentation
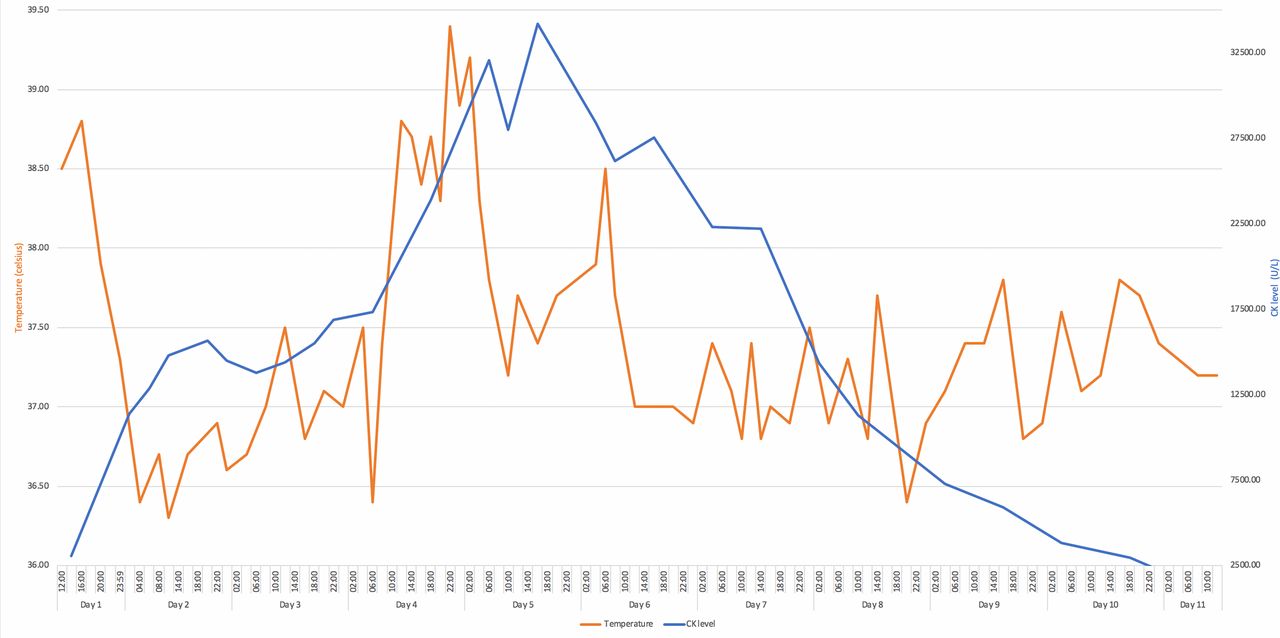
A man aged 29 years with a past medical history of cerebral palsy, seizures and chronic constipation that presented in late winter with 3 days of fevers, nausea, vomiting and anorexia. On physical examination, he had a temperature of 38.8°C, heart rate of 167 beats per minute, blood pressure of 75/62 mm Hg, respiratory rate of 30 breaths per minute and an oxygen saturation of 90% on 3 L/min of supplemental oxygen. The remainder of his exam was significant for bibasilar crackles. Labs were significant for lactic acid of 8.6 mmol/L (normal range 0.3–1.5 mmol/L), creatinine of 8.48 mg/dL (normal range 0.38–1.02 mg/dL) and total CK of 3043 U/L (normal range 0–200 U/L). Urinalysis revealed haemoglobinuria but only 3 red blood cells per high power field (normal range 0–5). Myoglobin in the urine was not assessed. CT of the chest showed patchy airspace opacities in bilateral upper lung fields. He was given intravenous fluids (IVF) and started on ceftriaxone, azithromycin and oseltamivir for suspected influenza and superimposed bacterial pneumonia. The patient defervesced the following day. PCR of a nasopharyngeal specimen was negative for viral pathogens, including influenza. Oseltamivir was stopped. Blood cultures were negative. Creatinine decreased to <1.5 mg/dL and lactic acid normalised. However, CK increased to 16 000 U/L over the next 2 days despite aggressive hydration (figure 1) while serum creatinine normalised.

{kind=link}
Temperature (°C) plotted with creatine kinase (CK) level over time (days).
On hospital day 4, the patient had recurrence of fever to 38.8°C and was tachycardic with intractable vomiting. Antibiotics were broadened to piperacillin-tazobactam and vancomycin. Nasopharyngeal swab for viral pathogens was repeated and was positive for influenza A, subtype H3. Oseltamivir 150 mg twice daily was initiated. Aspartate aminotransferase (AST) increased from 39 IU/L (normal range 0–37 IU/L) on admission to 119 IU/L. Alanine aminotransferase (ALT) decreased from 57 IU/L (normal range 0–50 IU/L) on admission to 43 IU/L. CK increased further to 23 867 U/L. Therefore, maintenance IVF was increased from 100 mL/hour to 250 mL/hour. CK peaked at 34 176 U/L the following day. Over the next few days, the patient finally defervesced and CK gradually decreased to 10 000 U/L. Blood cultures remained negative and all antibiotics were discontinued. Other causes for rhabdomyolysis were investigated and excluded. This patient was not on any medications that would precipitate rhabdomyolysis prior to admission. He had no seizures, trauma, prolonged immobility or heat exposure. There was no evidence of connective tissue disease. With supportive care and antiviral therapy, his CK levels declined further. The patient was discharged on hospital day 11. He completed a 10-day course of oseltamivir.
Differential diagnosis
There are traumatic and non-traumatic causes of rhabdomyolysis. Traumatic causes include crush injury, prolonged immobility, compression syndrome, excessive exercise and lightning injury. Non-traumatic causes include metabolic myopathies, sepsis, electrolyte abnormalities, medications such as statins and daptomycin, illicit drugs such as cocaine and methamphetamine, alcohol, hyperthermia or hypothermia and bacterial and viral infections.3
In our case, there were no physical examination findings or laboratory abnormalities that indicated another cause for rhabdomyolysis. The patient’s maximum temperature during the hospitalisation was 39.4°C, and prior to this measurement, the maximal temperature measured was 38.8°C, at which point serum CK level had already reached 20 000 U/L. Therefore, it was unlikely that hyperthermia was the aetiology for the rhabdomyolysis. Our patient did not drink alcohol or do illicit drugs. He did not take any medications regularly. He had no clinical signs of seizures. Hence, an electroencephalogram was not performed to exclude seizure as the aetiology. He required vasopressors briefly on day 1 of his hospitalisation making sepsis an unlikely cause of the rhabdomyolysis. Oseltamivir has also been implicated as a rare aetiology of rhabdomyolysis.4–6 In our case, the patient presented with an elevated CK level of 3043 U/L at admission making it less likely the inciting event. Furthermore, use of the Naranjo Adverse Drug Event Probability Scale indicated a doubtful relationship between rhabdomyolysis and oseltamivir therapy in this patient.7
A muscle biopsy ruling out an underlying metabolic myopathy or polymyositis to identify a risk factor for rhabdomyolysis was not obtained. The clinical picture suggested a diagnosis of virus-induced rhabdomyolysis.8
Treatment
Oseltamivir is used to treat influenza. It inhibits neuraminidase, which is an enzyme that helps release new viral progeny that reproduce within the host. It does not kill the virus but slows down the rate of infection within a person. It is recommended to initiate treatment within 2 days of the onset of symptoms to shorten the duration of the illness.9 Nonetheless, there is a significant mortality benefit even if therapy is initiated later. One study found a survival benefit in patients treated with neuraminidase inhibitor therapy compared with untreated patients (75% vs 58%; p<0.0001) when treatment was started within 5 days of symptom onset.10 Our patient received one dose of oseltamivir 75 mg empirically, which was stopped after the initial negative test. Oseltamivir 150 mg twice daily was resumed after a positive test on hospital day 4. At that time, the serum creatinine and creatinine clearance were 1.17 mg/dL and 86 mL/min, respectively.
The severity of the influenza pandemic of 2009 prompted WHO to advise that use of higher doses of oseltamivir (150 mg twice daily) and longer treatment regimens (longer than 5 days) should be considered when treating severe or progressive illness.11 Since 2009, other studies found no clinical benefit in higher dosing.9 12–15
The proposed mechanisms of acute renal failure in rhabdomyolysis include renal vasoconstriction, tubular cast formation, tubular ischaemia, direct heme pigment-induced cytotoxicity and free radical production among others.16 17 Therefore, the treatment for rhabdomyolysis is largely aimed towards prevention of further injury to myocytes by removal of any offending agents and large volume administration of isotonic IVF. The goal is to dilute the heme pigment as much as possible to prevent localised kidney ischaemia, increase renal perfusion and increase urine excretion of heme pigment and existing cast formations. The optimal type of fluid and rate of infusion is not known. The rate of IVF administration is generally titrated to a urine output of 200–300 mL/hour, while carefully monitoring the patient for signs of fluid overload and electrolyte abnormalities.
Bicarbonate-containing IVF can theoretically help to prevent hyperkalemia, protein precipitation in kidney tubules and correct acidosis.16 It is unknown if bicarbonate-containing IVF is superior to isotonic fluids in preventing acute renal failure. For severe rhabdomyolysis, renal replacement therapy may be needed, particularly if volume overload precludes large volume IVF administration, or if hyperkalemia, uraemia or acidaemia is present.
Outcome and follow-up
The patient in our case improved and at the time of discharge his kidney function was normal (serum creatinine 0.61 mg/dL) without needing any type of renal replacement therapy during the hospitalisation. Two weeks after discharge, a follow-up call was made and the patient was doing well.
Discussion
Rhabdomyolysis is characterised by breakdown of muscle tissue causing release of CK, aldolase, lactate dehydrogenase, ALT and AST into the blood. Prompt recognition is critical to prevent permanent renal injury. Common causes of rhabdomyolysis include trauma, excessive exercise, medications, metabolic myopathies, electrolyte disturbances, connective tissue diseases, toxins and infections.3 18–20 The most common cause of virus-associated rhabdomyolysis is influenza.8 21 22 In a case series of 18 cases of H1N1 influenza, 62% of patients had elevated CK levels above 200 U/L.2 In an adult study of 505 patients, it was found that higher CK levels at the time of admission were associated with renal failure, dialysis requirement, mechanical ventilation and increased length of hospital stay.23
Symptoms of rhabdomyolysis include muscle pain, muscle weakness and fatigue. Other clinical manifestations include dark urine, nausea, confusion, decreased urine output and metabolic derangements such as hyperuricemia, hyperkalemia and transaminitis. The onset is usually within the first week of onset of respiratory symptoms.
The mechanism of rhabdomyolysis in influenza infection appears to be due to direct viral invasion of myocytes.8 18 20 In a porcine model, it was found that muscle cells express sialic acid receptors similar to respiratory epithelial cells, which serve as binding sites for the virus.24
Furthermore, Desdouits et al studied the in vitro infectivity of influenza A, H1N1 subtype, to muscle cells from three healthy donors and found that the differentiated muscle cells were highly susceptible to infection and that progeny of those viruses were able to infect other muscle cells, suggesting that most or all of the viral cell cycle can be completed inside muscle cells in vitro.25 Interestingly, we observed a temporal correlation between fever spikes and a rise in serum CK level (figure 1). This predictable rise in serum CK occurred about 6 hours after a temperature spike. It is unclear what the precise mechanism is between the rise in the temperature and subsequent CK elevation but could be due to either direct viral invasion of myocytes or due to release of viral progeny following replication.
In our case, we had a negative influenza PCR initially. The overall sensitivity of PCR-based influenza test is high, ranging from 89% in a nasal swab specimen to 94% in a nasopharyngeal specimen.26 Timing is an important determinant of a test’s performance. A meta-analysis of 159 studies analysing the accuracy of different rapid influenza diagnostic tests showed a tendency towards higher sensitivity around days 2–3 since symptom onset, and a lower sensitivity on day 1 and day 4 and forward.27 In our case, the first specimen was obtained within 3 days of symptom onset making it less likely that poor timing was the cause of the initial negative result. The initial negative test was likely due to an improperly collected specimen. Prompt treatment was initiated once a diagnosis was made.
While it is recommended that treatment be initiated within 48 hours of symptom onset, studies show that patients with symptoms longer than 48 hours from influenza infection also benefit from treatment with oseltamivir. One study found a reduction in duration of symptoms by 1 day and decreased viral shedding when treatment was initiated within 3 days of symptom onset in influenza patients.28 Louie et al analysed data from 1950 patients admitted to an intensive care unit with pH1N1 influenza infection and found a survival benefit in patients treated with neuraminidase inhibitor initiation within 5 days compared with untreated patients (p<0.05 for each day 0–5).10 Viral shedding has been shown to be prolonged in critically ill admitted patients compared with those less severely ill, which could be why such patients benefit from therapy even if initiated 48 hours or longer after symptom onset. While these patients do benefit from delayed therapy, it is unknown if they benefit from higher doses of oseltamivir.
The mortality rate of rhabdomyolysis increases with increasing severity of the illness. One study reported 7.1% overall mortality in rhabdomyolysis which increased to 22.5% in patients with renal failure and 40% in those that require renal replacement therapy.29 Our patient did not require renal replacement therapy.
Our case highlights the need to consider checking CK levels in hospitalised patients with influenza infection. Additionally, influenza must remain in the differential for unexplained rhabdomyolysis.
Learning points
Influenza can cause severe rhabdomyolysis and clinicians should consider checking a creatine kinase (CK) level in adults hospitalised with acute influenza infection.
A correlation between fever and elevated CK levels may exist further supporting the hypothesis that direct myocyte invasion by the virus may be a key component of influenza pathogenesis.
Oseltamivir treatment has been associated with a reduction in mortality for acutely ill hospitalised patients with influenza up to day 5 after symptom onset.
References
Footnotes
Contributors All authors have contributed significantly to the final product of this article. All authors were part of the patient’s clinical care while in the hospital, contributed to the planning, data gathering, literature review, writing, editing and analysing the article. All authors have fulfill the criteria as defined by BMJ pertaining to authorship and all authors have approved the final version of this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.