Article Text

Abstract
Mycotic (infected) aneurysm involving the thoracic aorta is an exceedingly rare and life-threatening condition that is associated with high morbidity and mortality. We report an unusual source of Proteus mirabilis bacteraemia thought to be due to an infected aneurysm in the thoracic aortic arch in an elderly woman. Source of gram-negative bacteraemia is usually isolated to an intra-abdominal or a pelvic source. Proteus bacteraemia from an intrathoracic pathology is very uncommon, and in this case led to a delay in diagnosis. Although an infected aneurysm is a rare source of gram-negative bacteraemia, it must always be considered when common causes of bacteraemia have been ruled out especially in patients with vascular risk factors.
- vascular surgery
- infectious diseases
- cardiovascular medicine
- nosocomial infections
- pneumonia (infectious disease)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- vascular surgery
- infectious diseases
- cardiovascular medicine
- nosocomial infections
- pneumonia (infectious disease)
Background
Although only 1%–4% of all the arterial aneurysms are mycotic, they cause significant morbidity and mortality.1 2 We present a very rare case of Proteus mirabilis bacteraemia thought to have originated from an intrathoracic mycotic aneurysm. These infected aneurysms are more frequently seen in the femoral arteries and are commonly due to invasive procedures followed by mycotic aneurysms in the intra-abdominal region.3 4 Infected aneurysm involving the thoracic aorta is much less common and most published cases were due to non-typhoidal Salmonella species and Staphylococcus aureus.5–7 There was only one other case of thoracic-infected aneurysm due to Proteus bacteraemia reported in the literature.8
There are no standardised guidelines to treat infected aneurysms. Surgical treatment with extensive local debridement and re-vascularisation is considered to be the preferred option; however, this is associated with high morbidity and mortality.1 Endovascular aneurysm repair (EVAR) is becoming popular, particularly in patients who have a high surgical risk with a reported 2-year survival rate of over 70% reported with this procedure.9 10 A disadvantage of EVAR is that the infected aneurysm is left behind which could lead to recurrent infections warranting lifelong antibiotics and follow-up, and therefore this is considered a palliative approach.11 Our patient was treated with intravenous antibiotics together with thoracic endovascular aortic repair (TEVAR) with stenting, due to her age and other comorbidities.
Case presentation
An 81-year-old woman was initially admitted to cardiology unit for treatment of angina that was secondary to anaemia requiring blood transfusion. The admission was complicated with new-onset atrial fibrillation, which necessitated the initiation of anticoagulation therapy, following which she was discharged. She represented after 1 week with a 2-day history of fever with chills and rigours. Her other significant medical history included coronary artery bypass graft, congestive cardiac failure, infrarenal fusiform abdominal aneurysm (3 cm), hypertension with stage 3 chronic kidney disease and a 40 pack/year history of smoking. On examination, her temperature was 39.5°C. She did not have any peripheral stigmata of infective endocarditis. There was no history of thoracic trauma or having had an interventional procedure in the recent past. Auscultation of the precordium and lungs identified no murmurs, but there was reduced air entry on the left lung base. Her systemic examination was otherwise unremarkable.
Investigations
Blood tests showed a haemoglobin of 113 g/L, a white cell count (WCC) of 12.7×10 cells/L, a platelet count of 340×109 cells/L and an elevated C reactive protein (CRP) of 280 mg/L. Her international normalised ratio (INR) was subtherapeutic at 1.3. Chest radiography showed a small left pleural effusion with overlying consolidation, and her urinalysis showed only 1×106/L polymorphs.
One blood culture grew P. mirabilis, and the patient was treated with tazobactam/piperacillin (Tazocin), to which the organism was sensitive. Further detailed history to elicit the primary source of P. mirabilis bacteraemia, focusing on the urinary tract, abdomen, skin and respiratory tract or any device-related infections, did not reveal a source of the infection. On review of past records, no urinalysis was done during her cardiology admission. Subsequent further investigations were undertaken to help identify the source of gram-negative bacteraemia. A CT scan of the abdomen and pelvis did not show any anatomical abnormalities of the urinary tract or an intra-abdominal pathology to explain the bacteraemia. Transthoracic echocardiography (TTE) did not show any obvious vegetations, but it showed mild overall systolic dysfunction with possible inferolateral hypokinesis. We attempted a pleural tap on the left small effusion, but were unsuccessful. As a urinary tract and intra-abdominal source of bacteraemia were ruled out, the source of bacteraemia was presumed to be secondary to hospital-acquired pneumonia, which was in view of her most recent admission and the findings on her chest radiography. The patient improved clinically after a 7-day course of intravenous tazobactam and piperacillin, her CRP trending down to 17 mg/L.
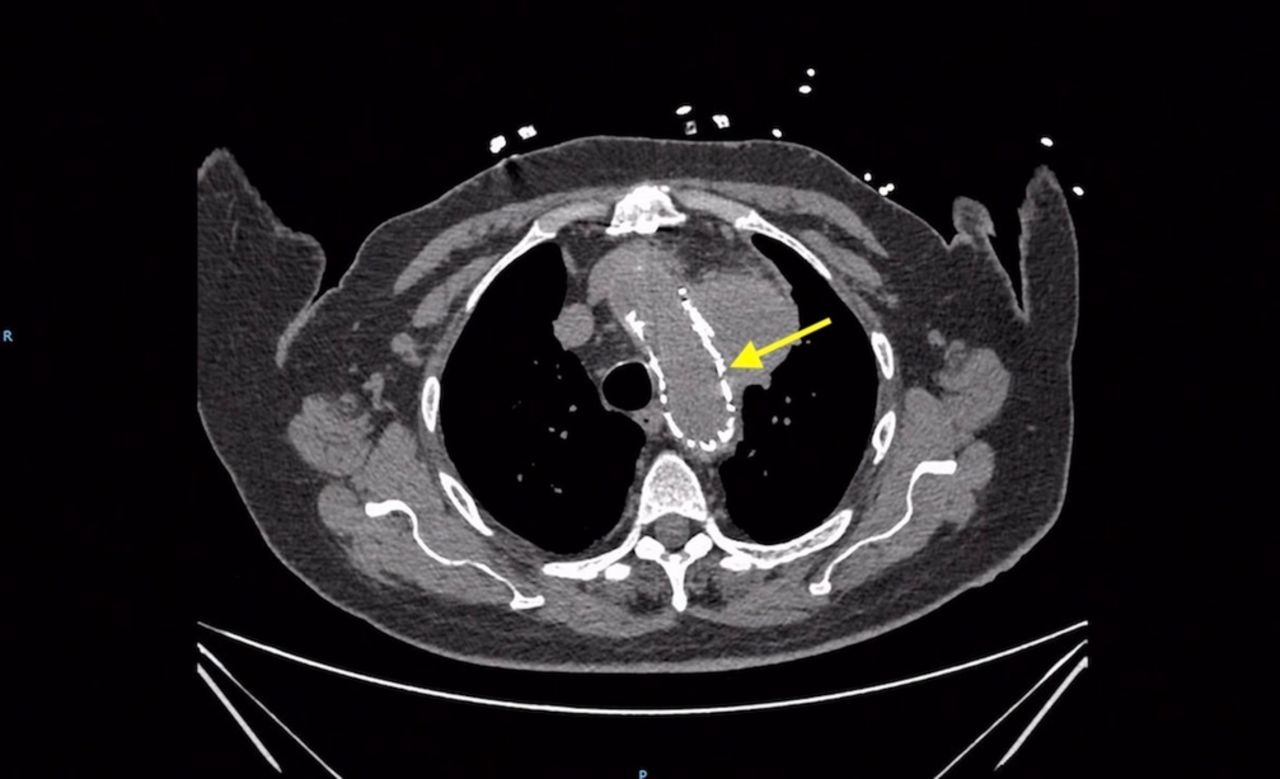
Ten days after discharge, she presented with left facial pain, hoarseness and high-grade fevers. A laryngoscopy confirmed left vocal cord palsy. An immediate cause of this vocal cord palsy was not apparent. A CT angiography (CT-A) of her thorax was then performed to determine the cause of her vocal cord palsy. This revealed a large saccular aneurysm (5.6×5.5×5.7 cm) with associated mediastinal fat stranding at the inferior aspect of the aortic arch (figure 1). The location of the aneurysm was just distal to the origin of the left subclavian artery extending out to the left side of the arch.

An axial CT angiography of the thorax showing a saccular aneurysm measuring 56×55×57 mm (arrow) with mediastinal fat stranding.
Differential diagnosis
The CT findings were very suggestive of an infected aneurysm of the aortic arch. We reviewed our initial diagnosis of pneumonia being the source of her P. mirabilis bacteraemia, as it is unusual for this to be originating from the respiratory tract. An infected aneurysm was considered a more likely source and there had likely been an antecedent infection of unknown origin, with direct seeding to an atherosclerotic thoracic aorta.
Treatment
The patient underwent thoracic endovascular aortic repair with stenting (TEVAR) the following day. A culture was not obtained from the aneurysm wall as an open repair was not performed. She was treated with intravenous tazobactam and piperacillin for 2 weeks, and this was subsequently changed over to a prolonged course of ciprofloxacin. During this period, her inflammatory markers trended down and her blood cultures remained sterile. The aneurysm on presentation was considered the most likely explanation for the Proteus bacteraemia, rather than it being a simple association. Her clinical improvement after TEVAR together with antibiotic treatment, improvement in inflammatory markers, subsequent negative blood cultures and initial radiological appearance indicate that she had an infected aneurysm.
Outcome and follow-up
Postoperatively, she had a complicated and prolonged admission due to non-ST elevation myocardial infarction and renal failure, which was managed conservatively. She was eventually transferred to a rehabilitation service where she made a good recovery.
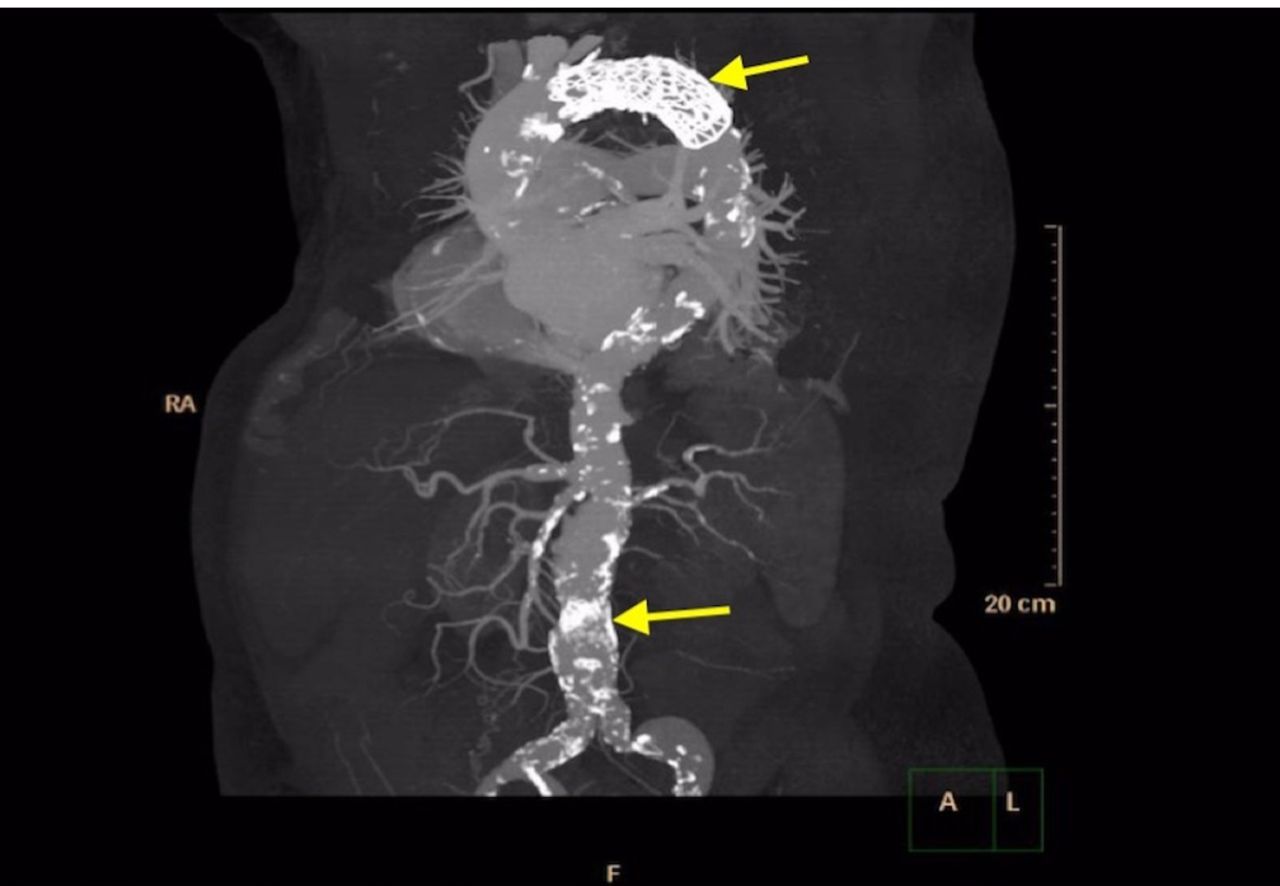
A CT angiography after -1 month follow-up (figures 2 and 3) revealed a stable sac size. The patient remained clinically stable.
An axial CT angiography of the thorax 1 month post-TEVAR showing a stable stent (arrow). TEVAR, thoracic endovascular aortic repair.

{kind=link}
{kind=link}
{kind=link}
One month post-TEVAR angiography showing a stable stent (top arrow) with evidence of widespread atherosclerotic calcified plaques in the descending aorta (bottom arrow). TEVAR, thoracic endovascular aortic repair.
Discussion
Mycotic (infected) aneurysms are focal and irreversible vascular dilatations that are caused by weakening and degeneration of the vessel wall, which is mostly due to invasive bacterial infection.12 They only cause 1%–4% of all arterial aneurysms but are associated with significant morbidity and mortality.1 2 They commonly affect any major arteries at bifurcations and tend to be more obvious if they involve the more superficial vessels (eg, femoral artery) and are harder to assess with deeper vessels.12 The femoral artery appears to be the most frequently involved artery and is associated with the use of more invasive intra-arterial monitoring and interventional procedures. The next most frequently involved arteries are those in the abdominal region.3 4 12
Mycotic aneurysm of the thoracic aorta is even rarer, and a few reported cases were mostly due to Salmonella spp.5–7 13 The mortality associated with mycotic aneurysm was high, ranging from 30% to 50%.13 The clinical outcome is especially poor in patients with infection caused by non-typhoidal Salmonella.5 13–15
The word ‘mycotic’ comes from the fresh fungus vegetation appearance of the aneurysms, and this term was first mentioned by Osler and was associated with bacterial endocarditis.16 17 Since the introduction of antibiotics, bacterial endocarditis as a cause of mycotic aneurysms is now present in only a minority of patients. The exception is intracranial mycotic aneurysms, which are exclusively due to endocarditis.12 18
The most common risk factors for developing infected aneurysms are atherosclerosis and old age, as seen in this case report.18 19 The pathophysiology is thought to be due to a direct intimal wall injury with susceptibility to bacterial seeding.12 18 20 Mycotic aneurysms could also arise due to septic emboli, direct bacterial inoculations,21 22 a pre-existing aneurysm, contiguous infection, antecedent infections or in an immunocompromised host.12 23 The patient in this case likely had bacterial seeding to an atherosclerotic thoracic aorta due to a previous transient bacteraemia during her cardiology admission. It is unclear where the initial cause of Proteus bacteraemia began, but it may have been from the urinary tract or a vascular source.
The clinical features of an infected aneurysm depend on the location. They commonly present with a painful, pulsatile and enlarging mass or a febrile illness with insidious onset, anorexia and lethargy.12 24 25 With disease progression, patients can develop bacteraemia, rupture and haemorrhage of the aneurysms.2 24
Deeper-infected aneurysms are harder to elicit, as a patient could present with minimal signs. These should always be suspected in elderly patients with vascular risk factors who present with unexplained bacteraemia. The patient in this case report presented with hoarseness, which is believed to be due to thoracic aortic arch aneurysm causing impingement of the left recurrent laryngeal nerve.26 27 Other clinical presentations of deeper infected aneurysms include gastrointestinal bleeding (due to an aorta-duodenal fistula),28 heart failure or massive haemoptysis.29 30
The most common microorganisms that caused infected thoracic aortic aneurysms were non-typhoidal Salmonella (57%) and Staphylococcus aureus (14%).7 13 Mycotic aneurysms from gram-negative microorganisms present with a higher incidence of aneurysm rupture and mortality compared with those from gram-positive microorganisms.31 This is thought to be due to bacterial seeding of a susceptible atherosclerotic aorta.17 20 32 A thoracic mycotic aneurysm is an extremely rare source of P. mirabilis bacteraemia, with only one case report being found in a literature review by Semba et al.8 Another case report of a mycotic aneurysm involving the internal carotid artery was also associated with P. mirabilis infection.33 Some case reports of gram-negative organisms associated with infected aneurysms include Pseudomonas, 34 Escherichia coli ,35 Haemophilus influenza 36 and Campylobacter. 37
After a detailed history and physical examination, a suspicion of an infected aneurysm should be followed up by laboratory and imaging studies. Laboratory examination typically reveals an elevation of inflammatory markers that include a total WCC, erythrocyte sedimentation rate and CRP. Blood cultures should also be obtained, and they are only positive in approximately 50%–75% of cases.38–40 A negative blood culture is not sufficient to exclude a diagnosis of an infected aneurysm, and a tissue sample for culture and Gram stain should be done when possible. In one review about 25% of patients with infected aneurysms did not have any pathogen identified.39
Imaging studies should include a TTE followed by a transoesophageal echocardiogram, when clinically indicated, to exclude bacterial endocarditis.12 CT-A is the test of choice. CT-A is more useful for diagnosing infected aneurysm compared with digital subtraction angiography and it has a sensitivity and specificity of over 90%.12 41 42 CT-A findings that are suggestive of an infected aneurysm include a multilobulated or a saccular aneurysm, soft tissue stranding, intramural air around the blood vessel and perivascular fluid collection.2 41–43 Magnetic resonance angiography is indicated if there is a contraindication to intravenous contrast and it is particularly useful for intracranial aneurysms.44
There are no standardised guidelines to help with the treatment of infected aneurysms. Proposed management strategies include a combination of antibiotic therapy with surgical debridement.12 13 43 On suspicion of an infected aneurysm, broad-spectrum antibiotic therapy should be used immediately to cover both gram-positive and gram-negative species and later tailored to culture and susceptibility results. Duration of treatment is based on clinical circumstances and a prolonged course of treatment (>6 weeks) may be warranted in the setting of an immunocompromised state, antibiotic-resistant organisms, persistently positive blood cultures and inflammatory markers that are slow to improve.43 45
Antibiotic therapy alone may control the bacteraemia but is associated with poor outcomes with reported in-hospital mortality rate around 50%.46 47 The role of surgery for an aneurysm which is infected follows the same principal as vascular graft infections, for which the aim is to remove the infected tissue to prevent further sepsis or complications that may arise from the aneurysm rupture.43 Morbidity and 1-year mortality rates in patients who underwent surgery were higher for patients with infected arch aneurysms compared with others sites of infected aneurysms.13 48
Endovascular aneurysm repair (EVAR) is emerging as a treatment alternative for infected aneurysms, with a 2-year survival rate of over 70% and EVAR has been successfully done in patients who are deemed as being high risk for open surgery.9 10 There is, however, concern of ongoing infection and surgical treatment should be considered for patients with aneurysm rupture or persistent fevers. Given the patient’s age and comorbidities in our case, EVAR was the preferred surgical option.
Pneumonia with an effusion is an unusual source for P. mirabilis bacteraemia and therefore we should have actively pursued a vascular source of infection prior to her discharge.49 In retrospect, we believe that Proteus bacteraemia, in this case originated from either the urinary tract or less likely from an intravenous cannula site during her cardiology admission, resulting in seeding of the susceptible atherosclerotic thoracic aorta.
Learning points
When the cause of the gram-negative bacteraemia remains elusive after preliminary investigations, one should actively look for vascular infections as a source especially in patients with significant vascular risk factors.
Pneumonia is an unusual source for Proteus mirabilis bacteraemia, and therefore the clinicians should actively pursue a vascular source of infection after excluding the common causes.
Mycotic aneurysms from gram-negative microorganisms present with a higher incidence of aneurysm rupture and mortality compared with those from gram-positive microorganisms.
The clinical outcome in patients with infected aneurysms is poor, especially in patients with infection caused by non-typhoidal Salmonella species.
References
Footnotes
Contributors SN: planned the case report and wrote the abstract, background, learning points and some parts of the discussion; also reviewed the overall manuscript multiple times and amended the discussion, case presentation and investigations; also added a number of references; also responsible for the patient consent form and all the communications with the patient; edited the figures. RB: wrote the case presentation and most parts of the discussion with references; also gathered figures for the case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.