Article Text

Statistics from Altmetric.com
Description
We present the case of a 60-year-old woman with gastric adenocarcinoma presenting for elective surgical resection. The patient underwent an uncomplicated distal gastrectomy with Billroth II reconstruction, and D2 lymphadenectomy.
On postoperative day 3, an upper gastrointestinal series showed interval progression of oral contrast into the colon. The patient was subsequently started on a liquid diet.
On postoperative days 4–6, the patient was unable to tolerate sufficient oral intake. A repeat upper gastrointestinal series was obtained (figure 1), with findings of obstruction of the efferent limb. The patient was taken for oesophagogastroduodenoscopy which demonstrated a stenosed Billroth II gastrojejunal anastomosis at the efferent limb site. The anastomosis was transversed, and a 2.3x10.5 cm WallFlex covered stent was placed under fluoroscopic guidance (figure 2).
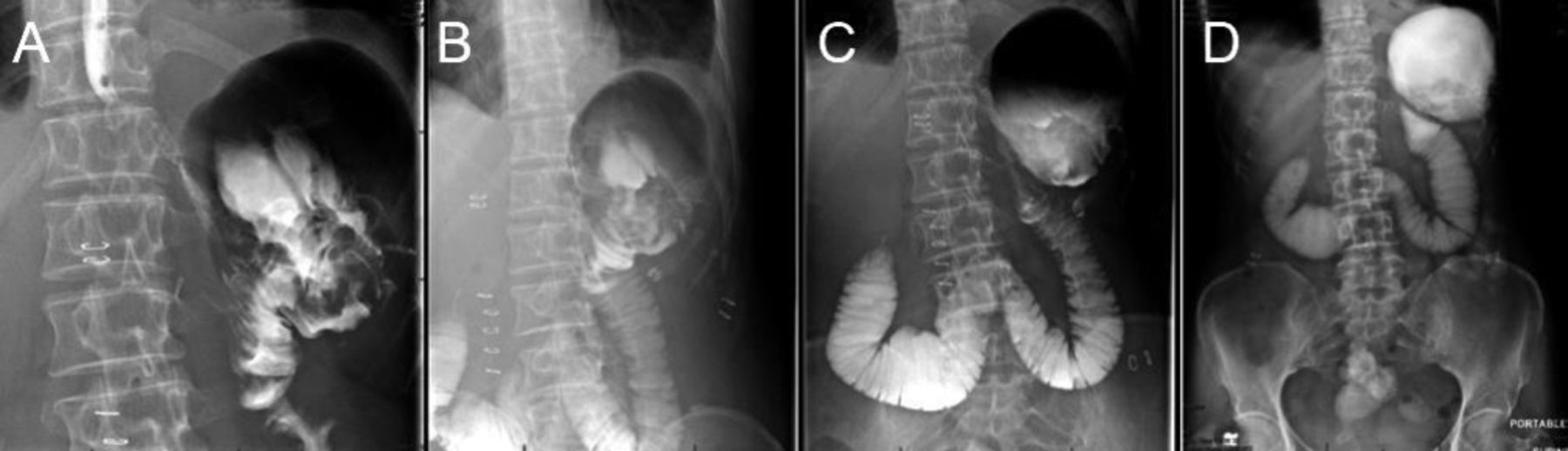
Upper gastrointestinal series with findings suspicious for obstruction of the efferent limb. (A) Passage of contrast through the gastrojejunal anastomosis. (B) However, essentially all contrast flows retrograde into the afferent limb, (C,D) with backflow into the stomach. No passage of contrast into the efferent limb.
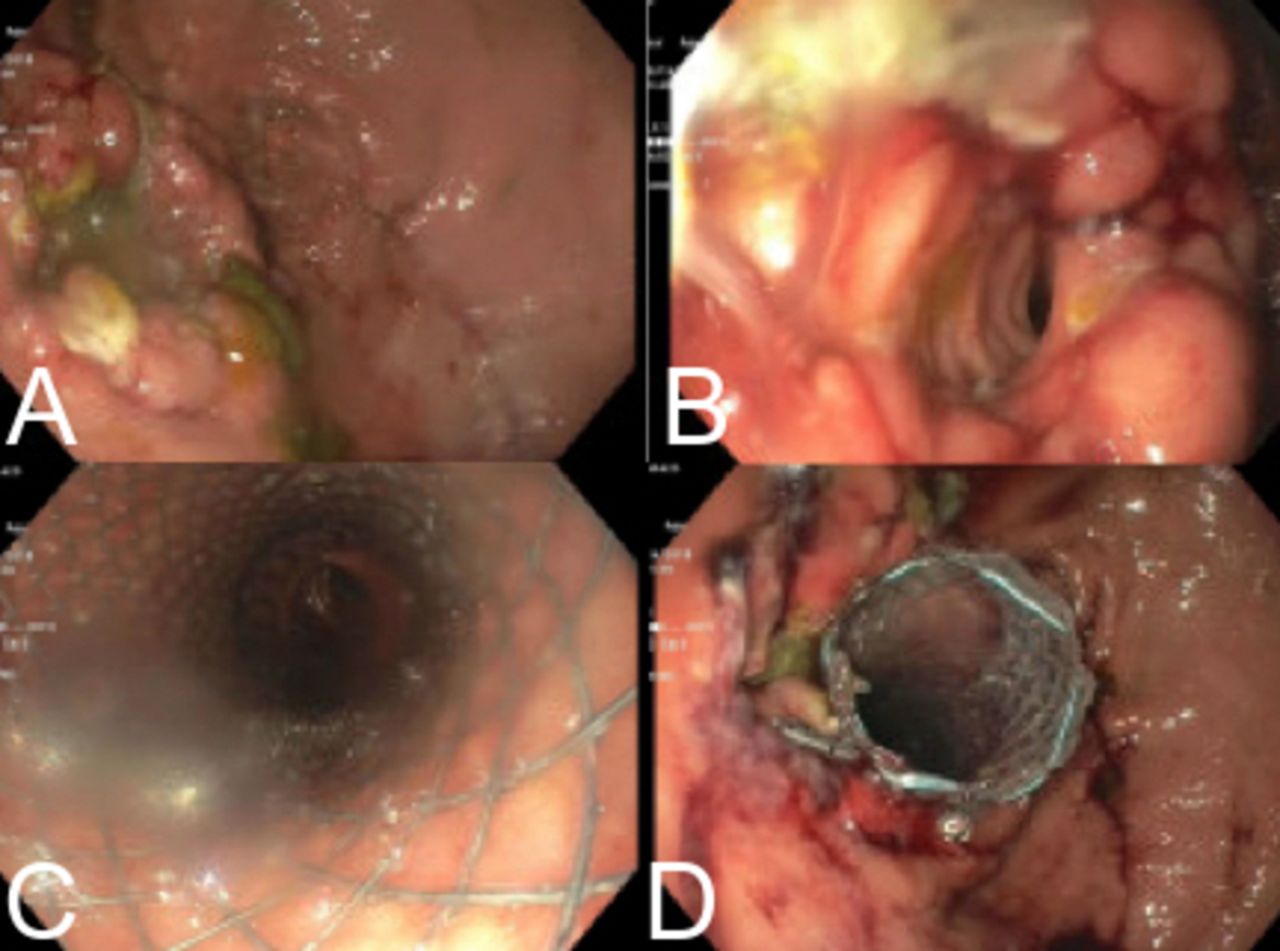
Endoscopic findings of the gastrojejunal anastomosis: (A) Bile seen but no apparent lumen. (B) Postintubation—angulation seen, with significantly narrowed lumen. (C,D) Poststent deployment—no angulation, widely patent.
Postprocedurally, a repeat upper gastrointestinal series was performed confirming a patent stent (figure 3). The patient’s diet was advanced and tolerated, and the patient was discharged home.

{kind=link}
{kind=link}
{kind=link}
Upper gastrointestinal series with prompt passage of contrast from the gastric remnant, through the endoscopic stent, and into non-distended small bowel and the right colon.
Efferent loop syndrome (ELS) is a rare complication defined as mechanical obstruction of the efferent enteric jejunal limb causing symptoms such as epigastric pain and massive bilious vomiting. ELS can occur with reconstruction of the alimentary tract after a Whipple procedure, Billroth II gastrectomy or Roux-en-Y gastric bypass. Gastrojejunal anastomotic stenosis rates in these types of surgeries range from 0.2% to 1.7%. However, these documented rates include the more common afferent limb syndrome and roux limb obstruction.1
The aetiology of ELS can be divided into early and late phases. Early phase causes include kinking and internal herniation, while late phase causes are predominantly caused by cancer recurrence.1 The mainstay treatment of ELS has historically been surgical intervention. However, with advancements in endoscopic procedures, there have been published techniques using metal stents, double pigtail stents and nasojejunal tube stents.1–3
Chang et al described the effectiveness of endoscopic stent therapy in the management of postoperative foregut surgery complications. They reported an 88.9% success rate in treating stenosis with the endpoint of being able to tolerate a diet.2 Stents are typically removed after 2 weeks, to minimise stent-related problems. Double pigtail and nasojejunal tube stenting have also been documented to have success rates as high as 95%.1 3
This case describes a rare postgastrectomy complication which was successfully treated with modern endoscopic stenting technique. Early diagnosis was essential, as the patient could not tolerate oral feeds, which could have lead to malnutrition. Endoscopic dilation is another option that could have been explored, but can lead to restenosis and require multiple endoscopic procedures.
Our management was guided by the principle that the obstruction was caused by oedema around the anastomosis. Temporary stent placement allowed for a less invasive approach, earlier resumption of oral intake, a shorter length of stay and treatment which required only two endoscopic procedures (placement and removal of the stent). With modern advancements in endoscopic techniques, patients with efferent limb syndrome are able to avoid the morbidity associated with operative repairs.
Learning points
There are two types of ‘loop syndromes’ which may occur after gastric surgery— afferent and efferent. Efferent loop syndrome is less common of the two. Both syndromes are characterised by a mechanical obstruction at the site of a gastrojejunostomy, causing obstruction of gastric emptying. It is difficult to distinguish between the two based on symptoms alone, however, both have historically required corrective surgical interventions.
The gold standard to diagnosing efferent limb syndrome is an upper endoscopy; however, radiographic imaging can aid in the diagnosis. Upper gastrointestinal series can be performed, which will demonstrate regurgitation of oral contrast into the afferent limb and gastric pouch.
Advancements in endoscopic technique and technology have provided a valuable approach to treating both ‘loop syndromes.’ Surgery to correct these issues is often associated with higher rates of morbidity and mortality, and prolonged hospitalisation. There have been several reports documenting significant benefits to the use of endoscopic metal stents, double pigtail stents and nasojejunal tube stents. Further studies are required to analyse the optimal use and efficacy of endoscopy when approaching both ‘loop syndromes.’
Footnotes
Contributors Conception and design, acquisition of data or analysis and interpretation of data: DL and KB. Drafting the article or revising it critically for important intellectual content: DL, KB and PS. Final approval of the version published: DL, KB and PS. Agreement to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved: DL, KB and PS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.