Article Text

Statistics from Altmetric.com
Description
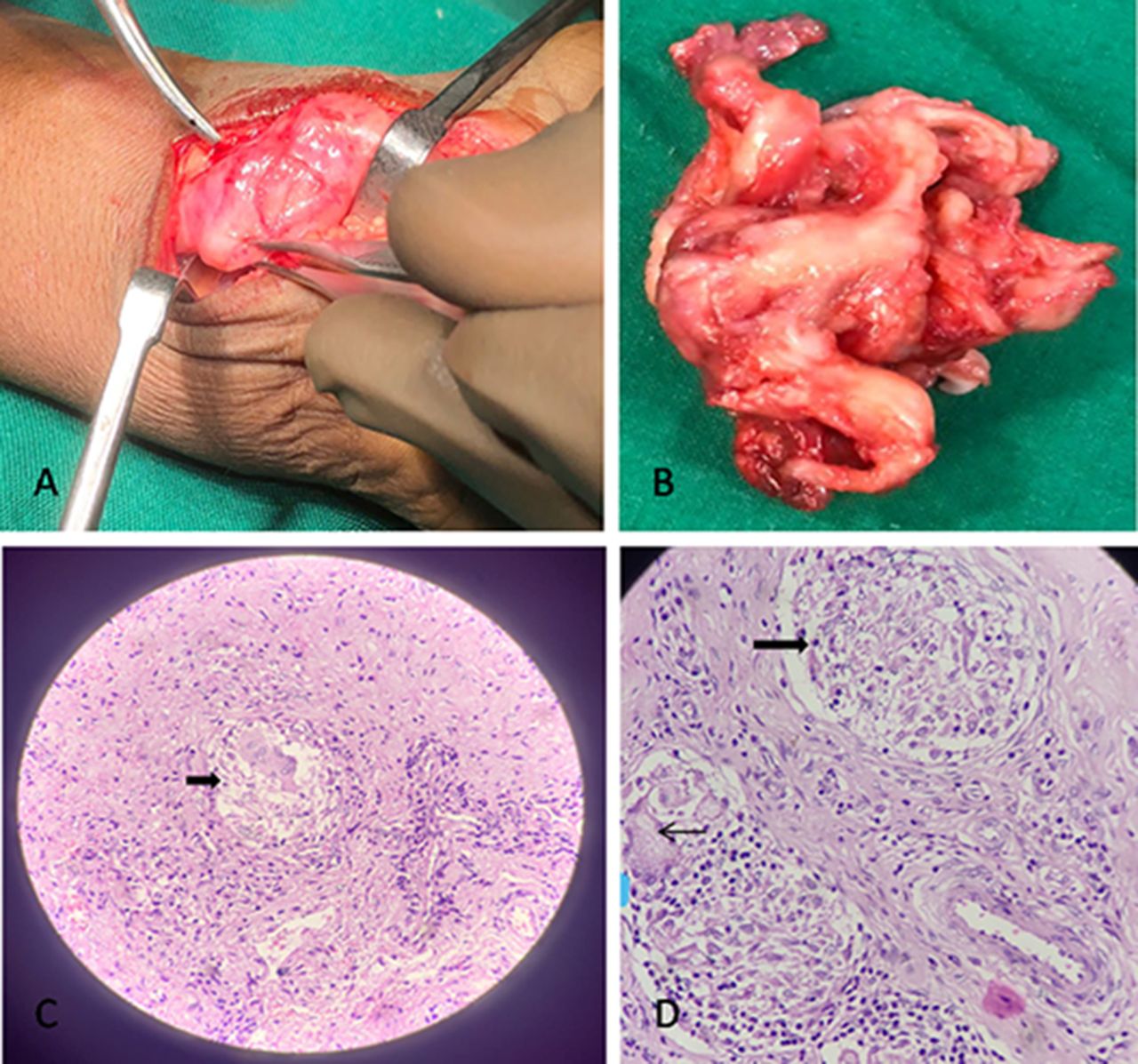
A man in his late 20s came to our hospital with progressive painful swelling of his left wrist (ventral aspect) for the last 6 months and loss of sensation in his index finger for last the 1 month. The swelling was pea sized initially and progresses to the present size of a lemon. On physical examination, the swelling was firm to hard in consistency and painful on touch/hand movements. The swelling was not mobile and the overlying skin was normal. There was no history of fever, trauma or any other chronic illness. An ultrasound examination of the wrist was performed which revealed excessive hypoechoic thickening of the tenosynovial sheath of flexor tendons causing compression over the median nerve (figure 1). A possibility of tenosynovitis was raised and an MRI examination was advised for a detailed evaluation of the soft tissue, bones and joints, which showed increased fluid intensity signal around flexor tendons with thickening of the synovial sheaths that was extending till the mid-palmar space. The carpal bones showed marrow oedema with few cystic changes in capitate and hamate; however, the joint spaces appeared normal (figure 2A–D). The median nerve was thickened and the normal fibrillar pattern was lost. These findings favoured infective aetiology and to relieve the nerve compression, the patient underwent surgery. Excision of entire swelling along with retinaculum sheath was performed (figure 3A,B) and the histopathological examination confirmed the lesion as tubercular tenosynovitis (figure 3C,D). The pathogen was found to be sensitive to all the standard antitubercular drugs and he was started on the standard antitubercular therapy. Postsurgery, the sensory symptoms resolved completely and he is on follow-up.

Ultrasonography greyscale image showing excessive hypoechoic thickening of tenosynovial sheath of flexor tendons.
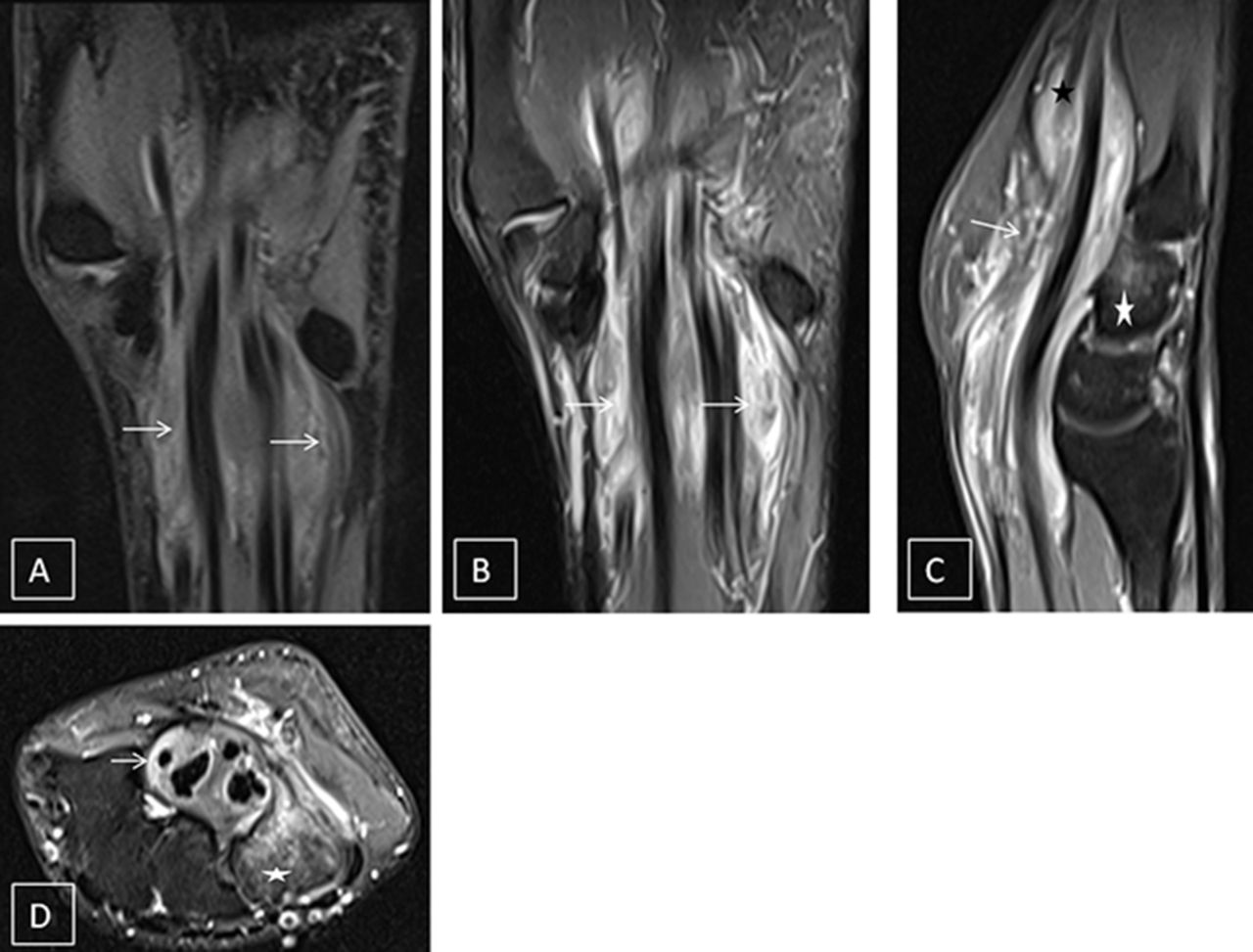
MRI of wrist joint: (A) Proton density fat suppressed (PDFS) image in the coronal plane and (B)PDFS sequence in coronal plane illustrating hyperintense signal along flexor tendons (white arrows) in the left wrist. (C) PDFS sequence in sagittal plane showing hyperintensity along the flexor tendon extending till mid-palmer space (black star) and marrow oedema in carpal bones (white star). Also, note the presence of fluid collection in the flexor sheath. (These images have been made by the author.) (D) Proton density fat suppressed (PDFS) image in axial plane showing synovial thickening (white arrow) andbone marrow edema (white star).
{kind=link}
{kind=link}
{kind=link}
(A and B) Gross intraoperative and postoperative images of excised swelling along with retinaculum. (C and D) Histopathology images in 10× and 40× power, respectively, showing granuloma formation (thick black arrows) and Langerhans giant cell (thin black arrow). (These images have been made by the author.)
Tuberculosis of the musculoskeletal system is very rare and presents in 10% of extrapulmonary tuberculosis. Atypical presentation of Tuberculosis includes spine (51%), pelvis (12%), hip and femur (10%), knee and tibia (10%), and ribs (7%); tuberculosis infection of the wrist is rare.1 Tuberculosis still remains the predominant cause of tendon sheath infection even though it is an uncommon site of extra-articular TB. Due to delayed presentation and overlapping features with other disease processes, the diagnosis is often delayed and the patient presents with secondary complications. Carpal tunnel syndrome, abscess formation, ulnar nerve compression, sinus formation, osteomyelitis or arthritis may occur as complications in these patients. The MRI is the ideal modality to diagnose this entity as well as to assess for any complications. The active disease appears as increased fluid signal intensities on T2/short-TI inversion recovery images on MRI. The synovial sheath appears thickened and elevated from the tendon due to the collection of fluid. The MRI also provides meticulous details about the complex wrist joint and hand spaces. This report discusses the imaging findings on MRI of a patient who presented with wrist swelling and was confirmed to have tuberculosis of the wrist on histopathological examination.1–3
Patient’s perspective
I am a labourer by occupation and had this swelling from a quite while, which was bothering me as I was not able to do my job properly because of this. Moreover, this swelling was increasing in size and there was a pain in it. I came to the hospital with this complaint and got relieved completely. Surgery went well and they called me after few days.
Learning points
Tuberculosis is one of the most common infective diseases in India. Usual sites of infection are the lungs and abdomen but isolated wrist involvement is rare; therefore, knowledge of tuberculosis and its different presentations is important.
MRI is the choice of modality for any musculoskeletal pathology as it provides high soft tissue resolution.
Ethics statements
Patient consent for publication
Footnotes
Contributors KS and RS contributed to the planning, conduct, reporting, conception and design, acquisition of data, or analysis and interpretation of data. SK and SG contributed to the acquisition and interpretation of the data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.