Article Text

Abstract
Despite advances and introduction of new therapies in the last decade, metastatic castration-resistant prostate cancer (mCRPC) has a poor prognosis. The development of androgen axis-targeted therapies such as abiraterone acetate, enzalutamide and darolutamide can prolong survival in mCPRC; however, resistance remains a barrier to prolonged response, necessitating exploration into resistance mechanisms and locoregional therapies. Here, we describe a patient with mCRPC that was progressing on abiraterone acetate. He was also found to have primary hyperaldosteronism from a functional adrenal adenoma, and thus he had a partial adrenalectomy to remove this tumour. Pathology confirmed an aldosterone-producing adrenal adenoma. After his adrenalectomy, he had a sharp decline in both his PSA (prostate specific antigen) and testosterone levels, and he enjoyed a year-long period of remission after his adrenalectomy. We propose several explanations for his response, the most likely being that his adenoma was producing both aldosterone and androgens. This is a unique case of mCRPC responding to partial adrenalectomy from a functional adrenal adenoma, and it raises insights that warrant further investigation into underlying mechanisms of resistance to androgen-targeted therapies.
- Prostate
- Urological cancer
- Prostate Cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The vast majority of deaths due to prostate cancer occur in men with metastatic castration-resistant prostate cancer (mCRPC), which refers to the failure of recurrent or metastatic disease to demonstrate response to androgen deprivation therapy (ADT). Men with mCRPC have a poor prognosis, with median survival times ranging from 1 to 5 years depending on a range of clinical and genomic characteristics.1–3 There are several proposed mechanisms of resistance to ADT, including amplification, splice variants and mutations in the androgen receptor, AR (androgen receptor) bypass pathways, increased de novo intratumoral androgen synthesis and increased intratumoral conversion of adrenal androgen precursors.4 5 In castration-resistant prostate cancer (CRPC), androgen precursors produced in the adrenal gland are increasingly converted to potent androgens through altered expression of steroidogenic enzymes.6–8 As early as the 1940s, cases of bilateral adrenalectomy in advanced prostate cancer had been shown to improve symptoms of metastatic disease, although with significant morbidity and mortality.9–11 More recently, non-surgical methods of ‘medical adrenalectomy’ that target adrenal steroidogenesis have been developed, including ketoconazole, a non-selective CYP17A1 inhibitor historically used off-label for CRPC,12 and abiraterone acetate, a selective inhibitor of CYP17A1 hydroxylase and lyase, enzymes expressed in testicular, adrenal and prostatic tumour tissue.13 Inhibition of this enzyme reduces circulating levels of androgens.
Abiraterone has demonstrated improved overall survival in mCRPC,14 and over the last decade, it has become a first-line systemic therapy option in mCRPC. Unfortunately, mCRPC typically progresses despite treatment with abiraterone and other first-line therapies. Here, we report a case in which a patient with progressive mCRPC while on abiraterone acetate had an extraordinary disease response and remission after partial adrenalectomy was performed for an incidental functioning adrenal adenoma. To our knowledge, this is first such case of an adrenal tumour contributing to castration-resistant disease and response of such disease to surgical resection.
Case presentation
The patient is an African American man who was first diagnosed with prostate cancer in his late 50s approximately 24 years ago, initially presenting with haemospermia and dysuria. An elevated PSA and abnormal digital rectal examination prompted prostate biopsy which revealed intermediate risk grade group 2 prostate adenocarcinoma in three cores. Open radical prostatectomy (RP) was performed, and pathology revealed tumour stage pT3b adenocarcinoma with bilateral extracapsular extension, seminal vesicle invasion and a Gleason score 4+3=7 or grade group 3 high-risk disease. Initial staging scans were negative for metastatic or nodal disease. His post-RP PSA was undetectable. Within 1 year, he had biochemical recurrence to 0.3, and he was treated with early radiation therapy. His PSA remained undetectable for years until it gradually and steadily increased, leading to the initiation of intermittent ADT approximately 14 years ago for non-metastatic hormone sensitive disease. ADT was continued for approximately 1 year, during which time his PSA was undetectable. However, when ADT was held, his PSA rose to 7.8 ng/mL, and restaging scans revealed new bone metastases approximately 10 years ago. He restarted continuous ADT, but he unfortunately developed mCRPC 4 years ago. As a result, abiraterone and prednisone were initiated. Unfortunately, his PSA continued to steadily increase to 24.27 ng/mL 3 months after abiraterone/prednisone initiation.
Investigations
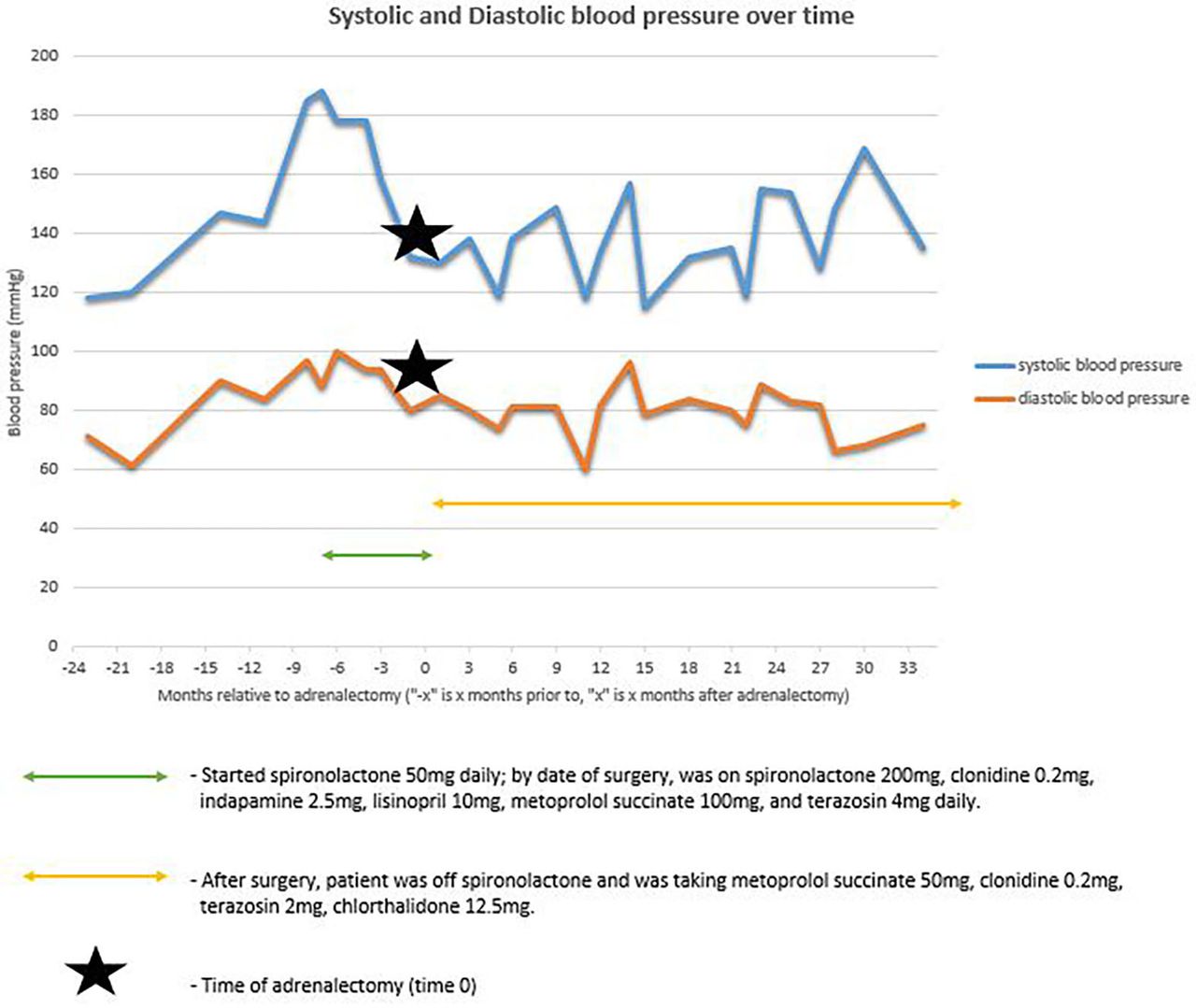
Incidentally, a right adrenal nodule was noted on CT imaging 4 years ago, measuring 0.7×0.9 cm. Given his worsening refractory hypertension requiring more than three antihypertensive therapies (figure 1) and chronic hypokalaemia, he was subsequently worked up for hyperaldosteronism. His plasma aldosterone level was found to be elevated at 58 ng/dL (reference range <21 ng/dL), and plasma renin activity depressed at <0.6 ng/mL/hour (reference range 0.6–3.0 ng/mL/hour), indicating primary hyperaldosteronism.

The patient’s blood pressure (in mm Hg) over time in months relative to the date of his adrenalectomy, which is represented by the black star. The green double arrow depicts the time period the patient was on certain blood pressure medications prior to his adrenalectomy, and the gold double arrow represents the time period the patient was on certain blood pressure medications after his adrenalectomy.
Treatment
Spironolactone was started at this time, and the decision was made to pursue a right adrenalectomy, completed 3 years ago, about 4 months after abiraterone/prednisone initiation. Histopathology revealed an adrenal cortical adenoma (figure 2), with findings consistent with an aldosterone-secreting tumour previously treated with spironolactone. His symptoms of hyperaldosteronism improved, leading to discontinuation of spironolactone after surgery.

(A) Low-power view of adenoma demonstrating a mix of eosinophilic cells and cells with cytoplasmic lipid (H&E, 100×). (B) High-power view of adenoma demonstrating lipid-rich cells with characteristic spironolactone bodies; intracytoplasmic eosinophilic inclusions with concentric laminations (arrowheads) (H&E, 400×).
Outcome and follow-up
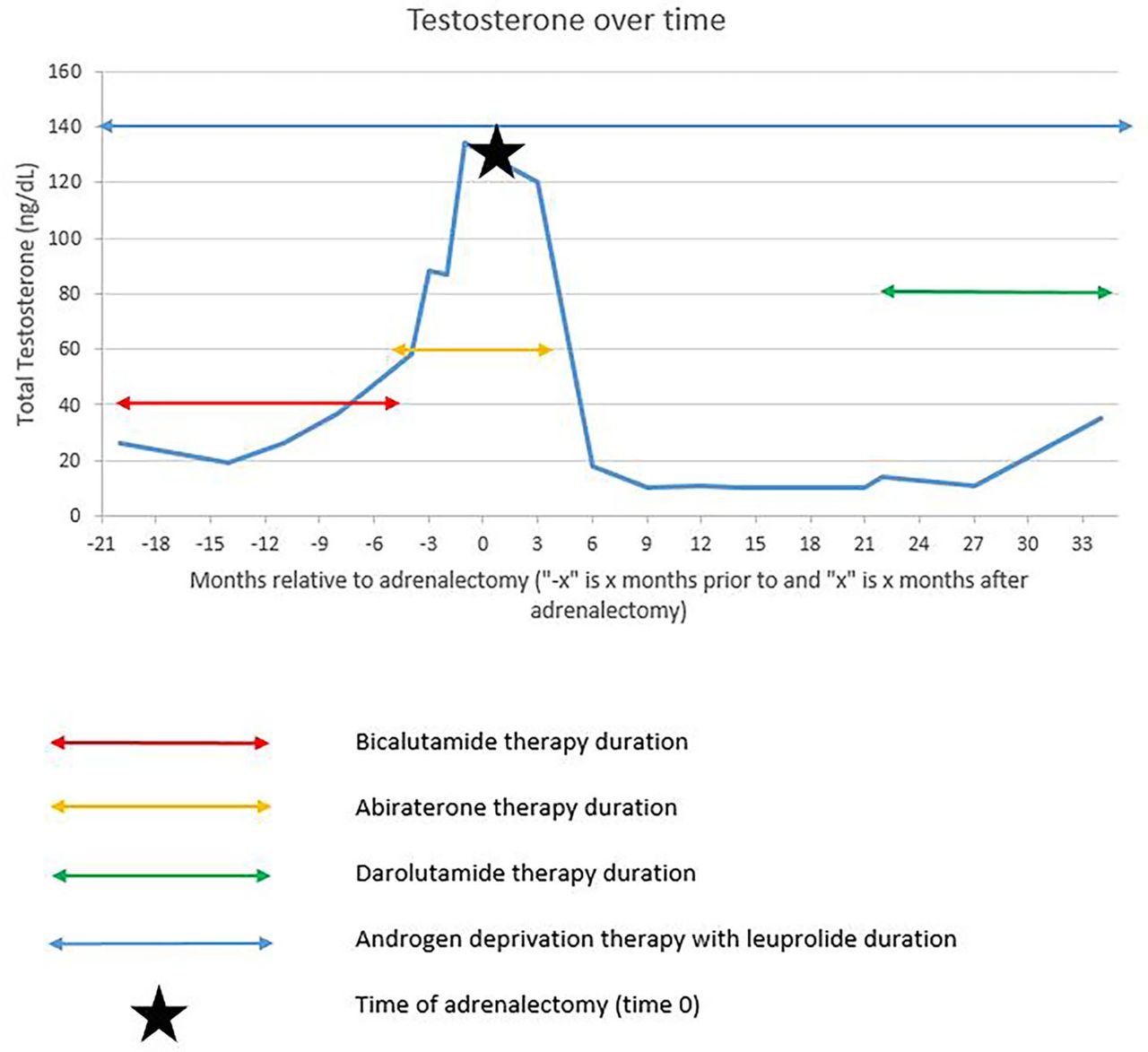
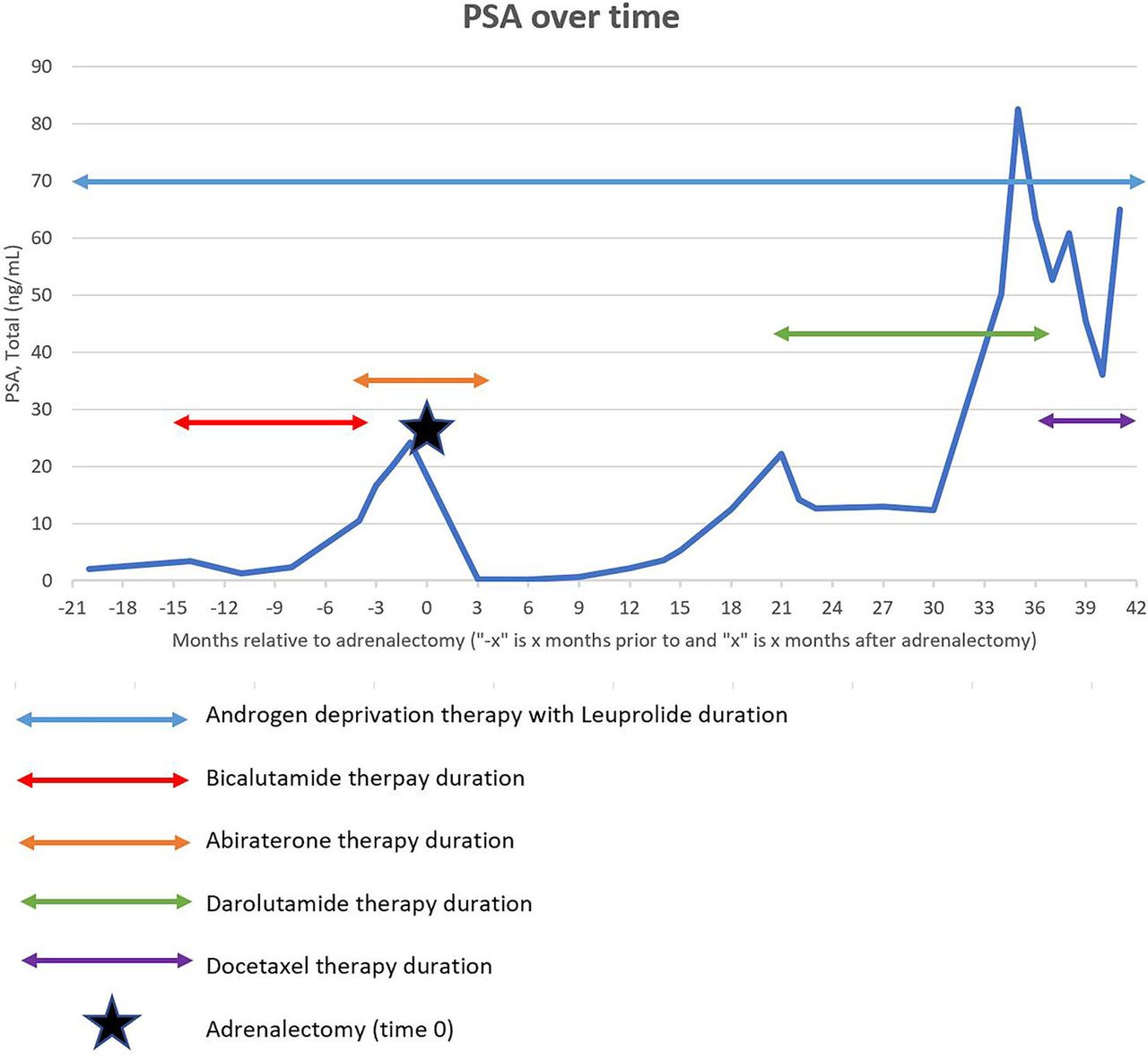
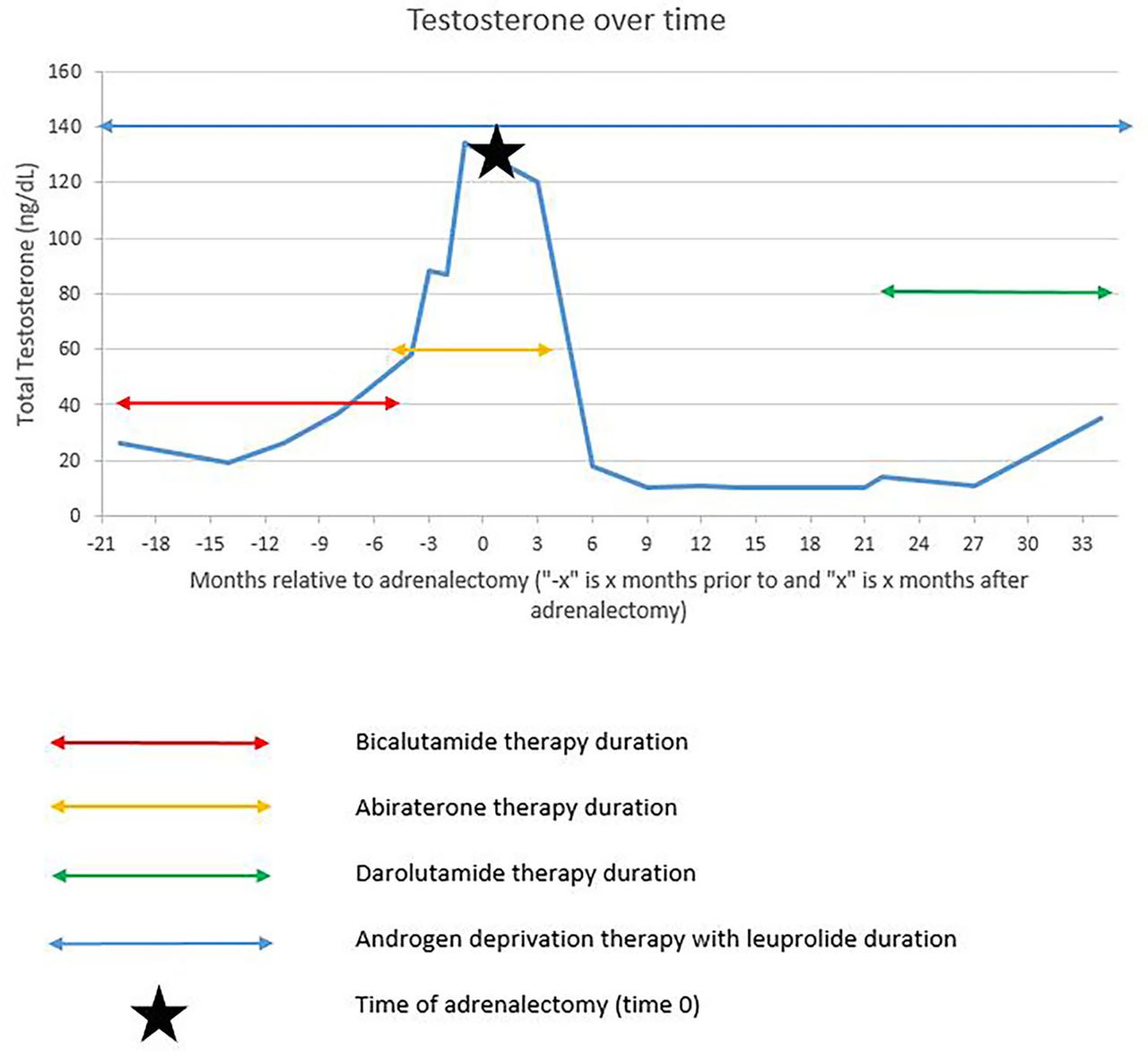
Interestingly, his PSA levels drastically decreased after right adrenalectomy. Three months after his adrenalectomy, his PSA dropped to 0.14 ng/mL (figure 3). Furthermore, his serum total testosterone levels, which were also monitored longitudinally, sharply decreased postadrenalectomy (figure 4), suggesting that the adrenal tumour was contributing to his serum androgen levels. The decision was made to discontinue abiraterone and continue with ADT monotherapy. His disease remained stable with PSA levels under 10 ng/mL until 1 year after adrenalectomy. Unfortunately, his disease eventually progressed again with bladder invasion of a local recurrence and progressive bone and lymph node metastases 2 years ago, requiring escalation of therapy. He was started on darolutamide, which stabilised his PSA levels until he progressed further 1 year later. He then switched to docetaxel, of which he has completed eight cycles. He was hospitalised on multiple occasions in the past 3 months for infectious and urinary complications related to his disease burden.

The patient’s serum total PSA (ng/mL) over time in months relative to the date of his adrenalectomy, which is represented by the black star. The coloured double arrows represent the duration of time that the patient was on certain therapies for his prostate cancer.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The patient’s total testosterone level (ng/dL) over time in months relative to the date of his adrenalectomy, which is represented by the black star. The coloured double arrows represent the duration of time that the patient was on certain therapies for his prostate cancer.
Discussion
Adrenal physiology is critical to the progression of prostate cancer as a contributor of serum androgens, and many prostate cancers take on an adrenal phenotype by upregulation of these adrenal androgenic enzymes and autocrine/paracrine synthesis and usage of androgens to survive the castrate state. There have been many advances in the treatment of mCRPC, with the introduction of new therapies and approaches in the last decade that target the androgen axis, including androgen-targeted agents like abiraterone acetate and AR targeting agents such as enzalutamide, apalutamide and darolutamide, which can prolong mCRPC patients’ survival. However, despite these positive initial responses, resistance remains a barrier to prolonged response in mCRPC. Cytotoxic chemotherapy such as docetaxel and cabazitaxel, immunotherapy such as sipuleucel-T and pembrolizumab, and precision therapies such as the targeted radioligand Lu177-PSMA-617 (Pluvicto) and PARP (poly ADP-ribose polymerase) inhibitors olaparib and rucaparib have been FDA (Food and Drug Administration) approved for prostate cancer.15–19 Even locoregional options such as surgery and radiotherapy are being explored in metastatic disease.19 Specifically, the PARP inhibitors laparib and rucaparib were FDA approved in 2020 for mCRPC patients with a pathogenic mutation in a homologous recombination gene, such as BRCA1 and BRCA2, bringing a survival benefit to this specific subset of the mCRPC patient population.17 18 Our patient has declined genetic testing up until now, but given his continued progression through docetaxel treatment, this will likely be pursued.
Here, we highlight an mCRPC patient progressing on abiraterone who demonstrated a response to adrenalectomy for a functioning adrenal adenoma. Before his adrenalectomy, his PSA and testosterone levels were sharply rising on abiraterone, implying his disease responded to the adrenalectomy rather than abiraterone. This is also supported by his continued relative PSA stability seen after abiraterone was discontinued and the sharp reduction in serum testosterone observed postadrenalectomy. As previously mentioned, bilateral adrenalectomy has been shown to improve symptoms of metastatic prostate cancer as early as the 1940s.9–11 There have been few case reports describing patients with both prostate cancer and adrenal tumours. Alikhan et al reported a case of advanced prostate cancer and a pheochromocytoma, although they did not comment on the effect unilateral adrenalectomy had on the prostate cancer.20 Navani et al described a patient with both mCRPC and metastatic androgen-secreting adrenocortical carcinoma who responded positively to left adrenalectomy,21 and Ashrafi et al reported a patient with CRPC with metastasis involving the adrenal gland that had a durable response to adrenal metastasectomy.22 As far as we know, this is the first reported case of mCRPC on a potent AR inhibitor like abiraterone, who responded positively to the removal of a functional adrenal adenoma.
Biochemical and clinical evidence support that our patient had an adrenal adenoma that secreted aldosterone and perhaps androgenic precursors. Given abiraterone acetate can cause secondary hyperaldosteronism,23 it is important to note that the elevated plasma aldosterone concentration and depressed plasma renin activity were identified before abiraterone therapy was initiated. In the setting of mineralocorticoid excess from abiraterone therapy, mineralocorticoids have been shown to inhibit androgen-induced AR conformational change, AR transcriptional activity and prostate cancer cell growth, suggesting therapies derived from mineralocorticoids may exert positive effects in prostate cancer.24 This is unlikely to be contributing in this patient, as the withdrawal of both excess aldosterone and androgen production after adrenalectomy was associated with prostate cancer remission.
The durable response seen after surgery raises the possibility that aldosterone could have been contributing to disease progression, as has been suggested in preclinical models in both renal and prostate cancer.25 26 A Canadian retrospective cohort study that examined thousands of men with heart failure found that spironolactone exposure significantly reduced the incidence of prostate cancer; this could be due to spironolactone’s known antiandrogen effects, but aldosterone antagonism could play a role in prostate cancer prevention and possibly treatment.27 This needs to be investigated further with more rigorous preclinical and clinical studies, but it offers a possible explanation for the response seen in this patient. The combination of spironolactone and abiraterone could have also been a contributing factor. Spironolactone has well-known antiandrogen activity, but studies have proposed a possible positive androgenic effect of the drug,28 particularly in an androgen-deprived environment, like that created by abiraterone. Several case studies have described the negative effect the combination of spironolactone with abiraterone has on mCRPC.29–32 In this case, it is difficult to determine whether the medication combination withdrawal or the adrenalectomy itself is responsible for this patient’s response, as spironolactone was discontinued at around the same time as his adrenalectomy. Additionally, serum testosterone levels clearly declined postadrenalectomy, which do not explain the spironolactone effect. Either way, this potential drug interaction is important to study further, as spironolactone is a common medication for indications such as heart failure and cirrhosis, conditions with significant patient population overlap with prostate cancer.
Finally, the patient’s adenoma was likely secreting testosterone in addition to aldosterone. Examining the patient’s total testosterone trends while on ADT, there is a rise in testosterone levels leading up his adrenalectomy, followed by a sharp drop after the date of his adrenalectomy. As seen in figure 4, he had almost 2 years of stable testosterone levels after his adrenalectomy, after which these levels started to uptrend. This is likely because of his disease progression. His total testosterone levels are overall decreased given treatment with ADT; however, this trend raises the question of whether this adrenal adenoma was also androgen-secreting, which would have contributed to his durable PSA response after adrenalectomy. Unfortunately, we did not obtain preadrenalectomy functional labs to determine if there were increased circulating adrenal androgens. Nevertheless, cosecreting adrenal tumours producing both aldosterone and androgens, although very rare, have been reported in the literature. Peppa et al described a patient with adrenocortical carcinoma secreting aldosterone, cortisol and androgens, while Schmitt et al described a paediatric patient with a functional adrenal adenoma secreting aldosterone and androgens.33 34 Because this patient was on ADT for his prostate cancer, the symptoms classically associated with androgen-secreting tumours were not observed. However, the trend suggests his adrenalectomy contributed to the decrease in serum testosterone levels, and perhaps a cosecreting adrenal adenoma producing both aldosterone and androgens is the explanation.
Learning points
Here, we describe a unique case of an African American man with metastatic castration-resistant prostate cancer (mCRPC) progressing on abiraterone that responded to partial adrenalectomy for an aldosterone-producing adrenal adenoma.
We discuss several potential drivers of disease response, including withdrawal of excess aldosterone, testosterone or spironolactone after the adrenalectomy—it is possible that a combination of the three contributed to this patient’s therapeutic response of his mCRPC disease to surgery.
Further investigation is warranted to understand the underlying mechanisms of resistance to androgen-targeted therapy. These insights have the potential to affect management in mCRPC and contribute to improved patient outcomes.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors KNS drafted large portions of the manuscript, contributed figures 1, 3 and 4, and revised the manuscript. MKL devised key concepts and revised the manuscript. XSJ contributed figure 2 and revised the manuscript. AA devised the overall concept of the manuscript (including case selection), drafted portions of the manuscript and revised.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.