Article Text

Abstract
A man in his 70s presented to the emergency department with a 3-day history of confusion and right-facial droop. He was diagnosed with stage IIIB (T4N2M0) malignant mesothelioma 6 months previously for which he was being given palliative chemotherapy. An MRI of the brain demonstrated a left parietal cerebral metastasis with unique radiological characteristics termed ‘donut sign’. He underwent a craniotomy and complete macroscopic resection of the lesion with a good postoperative outcome. Mesothelioma cerebral metastases are a rarely reported clinical entity, with only a handful of case reports and case series available. On MRI they often demonstrate a distinctive thick-walled lesion, termed ‘donut sign’, that may be indicative of the diagnosis. Furthermore, case autopsy series suggest these metastases may be underdiagnosed in the clinical setting due to the dismal prognosis. With newer and more effective neoplastic treatment strategies emerging, there may be a rising incidence of central nervous system metastases in the future.
- Neuroimaging
- Neurooncology
- Neurosurgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Central nervous system (CNS) metastases from malignant mesothelioma are a rarely encountered clinical entity. The scarcity of reported cases has meant that there is a poor overall understanding of their clinical and radiological phenotype. In the limited reports available they generally portend a dismal prognosis with a high rate of recurrence after resection. Furthermore, postmortem studies indicate that cerebral metastases of mesothelioma present significantly more commonly in autopsy studies than through clinical encounters.1 This may be related to a combination of the limited life expectancy of malignant mesothelioma as well as a lack of clinician awareness of the potential of cerebral metastases. As the prognosis of mesothelioma patients improves with emerging therapies, there may be an increased reporting of cerebral metastases along with a need for improved understanding of the clinical entity.
We present a rarely encountered case of cerebral mesothelioma metastasis that is treated with surgical resection and adjuvant radiotherapy. The case demonstrates the unique radiological characteristics along with the histopathological correlation of the metastasis. We describe the successful surgical management along with the perioperative clinical course.
Case presentation
A man, ex-plumber, in his 70s presented with a 3-day history of confusion and right facial droop. This was on a background of stage IIIB (T4N2M0) malignant lung mesothelioma diagnosed 6 months prior. The patient had received palliative radiotherapy and a Video-assisted thorascopic surgery (VATS) pleurodesis for refractory malignant pleural effusions. Notably, the patient also had developed SVC obstruction and was being managed with rivaroxaban after an SVC stent failed.
On examination, the patient was found to be oriented, had a fluent conversation and evidence of receptive dysphasia. He had a right-sided facial droop, of upper motor neuron character. He also had features of Gerstmann’s syndrome including acalculia, agraphia and left-right disorientation.
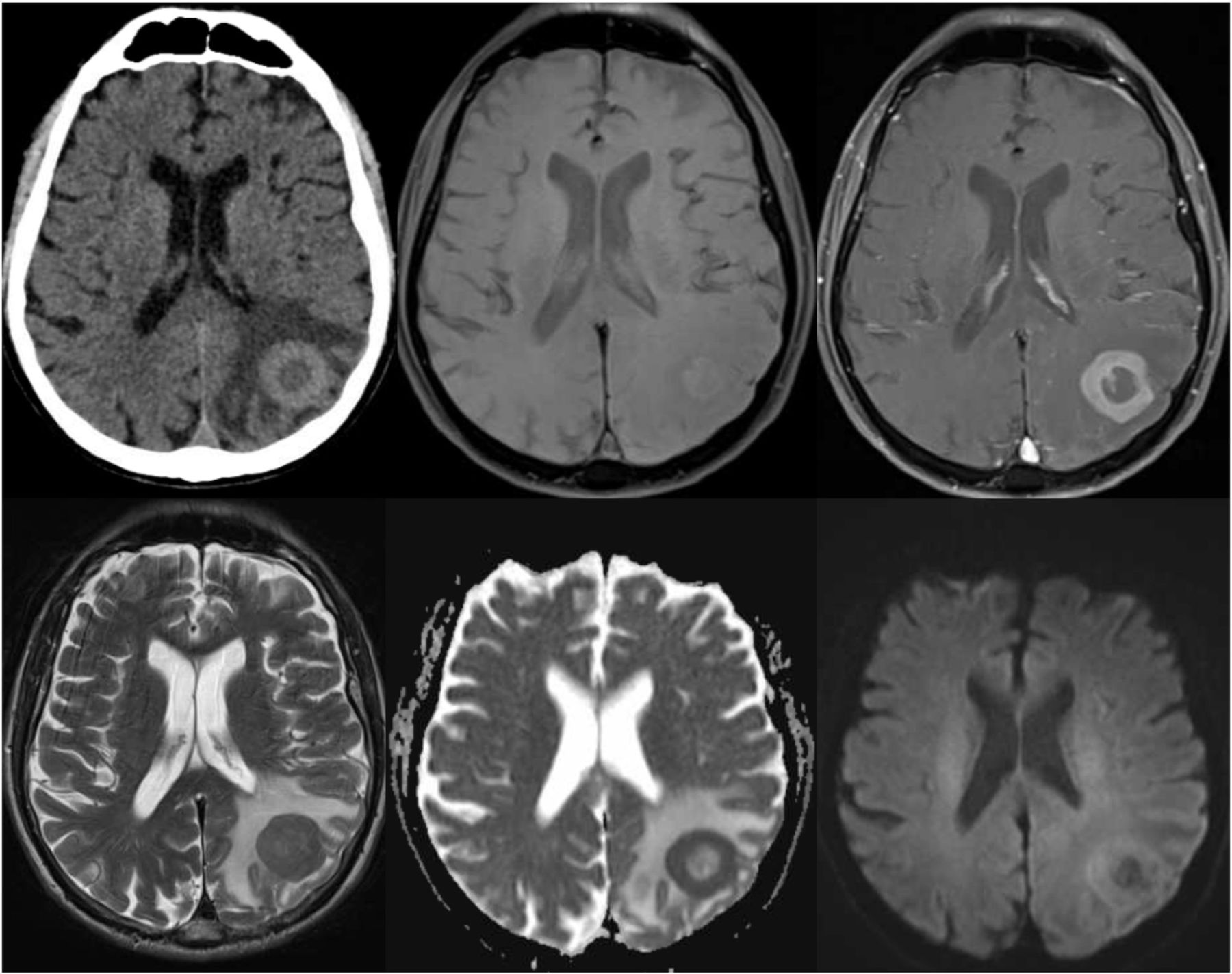
CT of the brain with contrast revealed a 28 mm diameter, thick-walled, round, left parietal mass lesion with surrounding oedema (figure 1). An MRI of the brain revealed the lesion to have a homogenously enhancing ring that was uniformly thick around the circumference and a central necrotic component that was T2 hypointense (figure 1). There were uniformly low-Apparent diffusion coefficient (ADC) values throughout the thickened wall.

Neuroimaging demonstrating the left parietal lesion. Top row (left to right) demonstrates CT brain (CTB), MRI-T1, MRI-T1 with gadolinium. Bottom row (left to right) demonstrates MRI-T2, MRI-ADC, MRI-Diffusion-weighted imaging (DWI).
Treatment
The patient was started on high dose dexamethasone along with a proton-pump inhibitor. After discussion with the patient and his family, and a brief period off rivaroxaban then patient was planned for surgical resection. The patient underwent a stereotactic craniotomy and resection of the left parietal tumour with complete macroscopic resection. At surgery, a well-defined, intra-axial tumour was encountered that was tan-yellow, lobulated and of hard-rubbery consistency.
Outcome and follow-up
The patient had no new postoperative deficits. There was mild ongoing receptive dysphasia; however, it was improved from preoperatively. He had an unremarkable postoperative stay and was discharged home to the care of his wife on day 3 postoperatively.
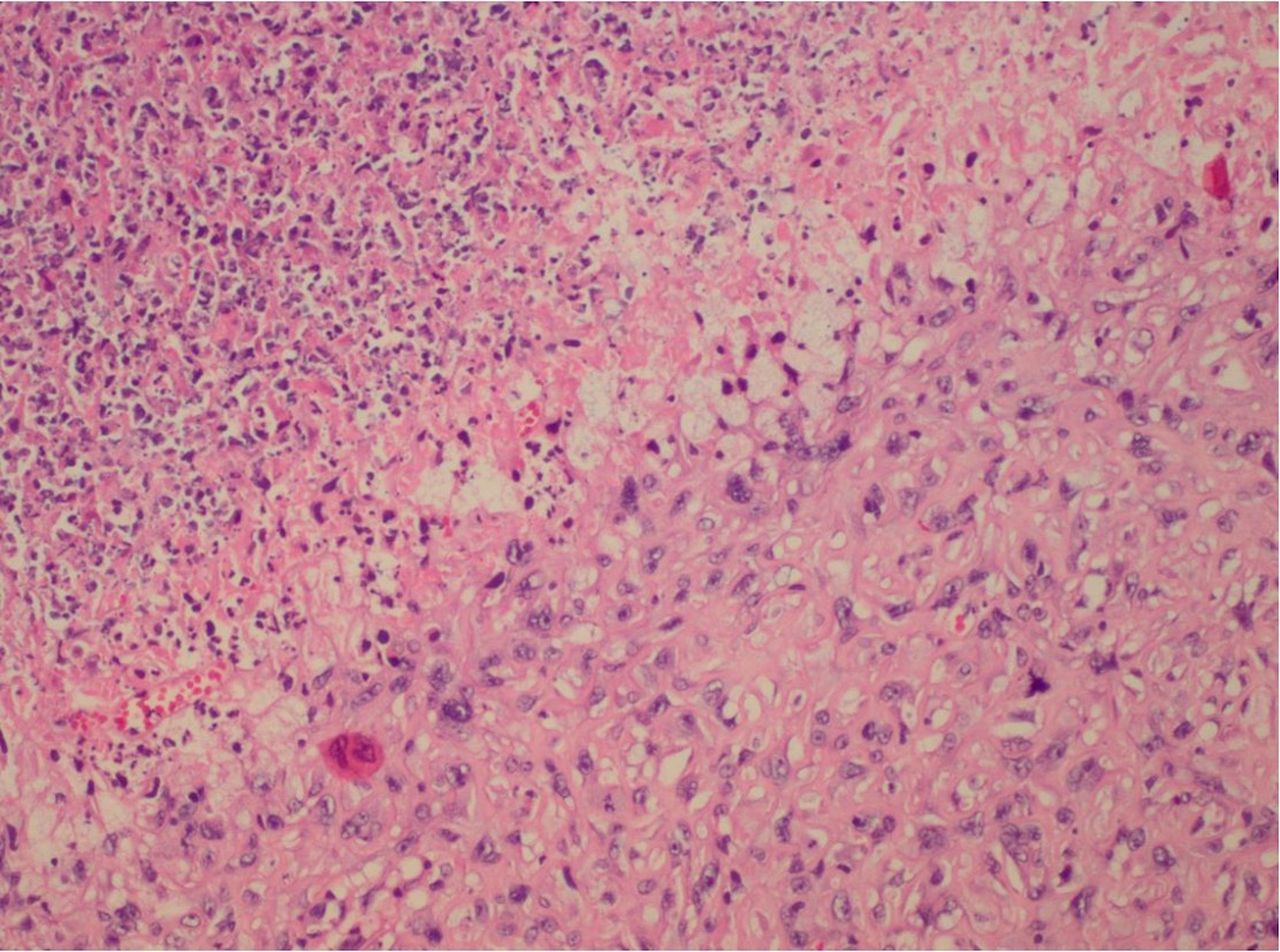
Histopathological analysis revealed a lesion consistent with malignant mesothelioma (figure 2). There were sheets of neoplastic cells with large, irregular, vesicular nuclei and prominent nucleoli, evidence of necrosis and a high mitotic rate. Immunostaining was positive for keratin AE1/AE3 and keratin 7, patchy calretinin and D2-40, weakly positive GATA3, ERG, non-specific HBME and vessel predominately staining WT1.

H&E section shows large malignant cells with round to ovoid nuclei and prominent nucleoli arranged in sheets with adjacent necrosis.
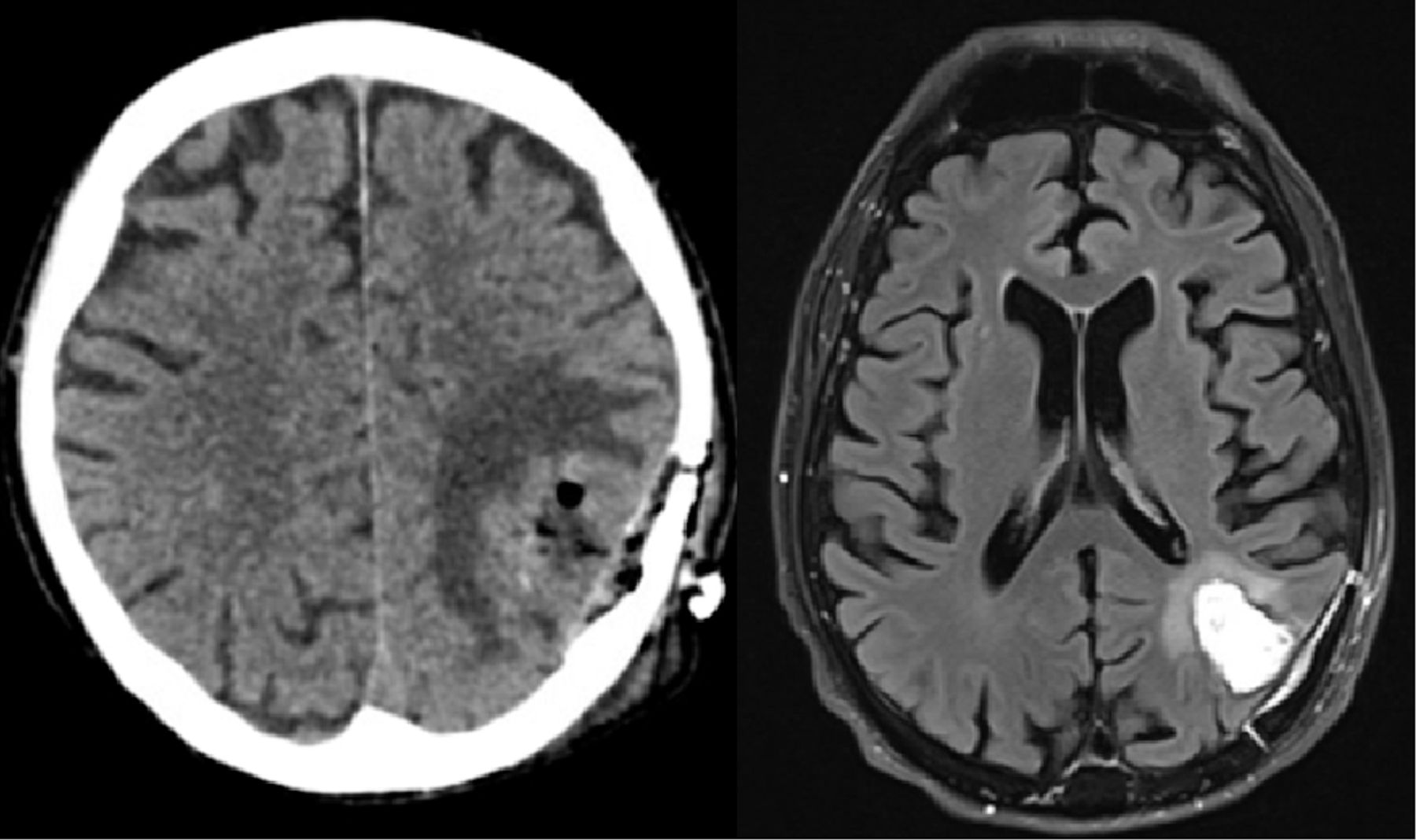
As is routinely performed in our unit, a CT of the brain was performed on day 1 postoperatively which showed no evidence of postoperative haemorrhage (figure 3). Furthermore, a radiotherapy planning-MRI at 1 month postoperatively demonstrated a fluid-filled cavity that did not demonstrate evidence of residual disease (figure 3).

{kind=link}
{kind=link}
{kind=link}
(Right) Axial plane Fluid-attenuated inversion recovery (FLAIR) MRI, 1 month postoperatively. Image shows a fluid-filled cavity with no indication of residual or recurrent disease, following macroscopic resection of the lesion. (Left) Axial CT scan of the brain 1 day postoperatively displaying no evidence of haemorrhage.
He was reviewed in the outpatient neurosurgical clinic at 4 weeks postoperatively and had made an excellent recovery. Apart from occasional forgetfulness, he had no neurological deficits on examination. He was living at home with his wife, independently mobile and able to attend to all activities of daily living. He was an ECOG 1. The patient went on to receive local radiotherapy through stereotactic radiosurgery. Furthermore, he completed a course of immunotherapy agent ipilimumab, as directed by the oncology team.
Discussion
CNS mesothelioma metastases are a uniquely rare event with a paucity of literature describing their clinical features. Mesothelioma is a cancer arising from the serosa lining surfaces of the body.2 This is most commonly of pleural origin; however, it also rarely originates from other serosal surfaces such as the peritoneum, pericardium or the tunica vaginalis. Mesothelioma is generally associated with a poor prognosis, with a median overall survival of around 12 months which is related to the histological subtype. The limited life expectancy associated with mesothelioma has likely influenced the rarity of clinical presentation with CNS metastasis and our consequent poor understanding of the entity.
Mesothelioma generally spreads by local invasion of surrounding structures from the primary site.1–3 Haematogenous spread is comparatively uncommon, and when it occurs it mainly results in bony metastases. The development of distant CNS metastases occurs similarly through haematogenous spread of the disease although it is exceedingly rare. Indeed, reported cases of CNS metastases are limited to a handful of case reports and small case series in the literature.3–5 One recent systematic review of the literature reported only 26 cases.1 This disproportionate aversion to spread to the CNS comparative to other sites of haematogenous spread may relate to underlying protective physiological mechanisms such as the blood-brain barrier.
Within the limited available literature that these cases are reported, the prognosis is generally poor and limited to weeks to months after diagnosis of CNS metastases.1 Treatment options most employed involve surgical resection followed by radiotherapy.
Moreover, due to the rarity of these lesions, there has been a paucity of literature describing the radiological features that may be unique to mesothelioma metastases. Typical MRI features of cerebral metastases include hypointensity in T1 and hyperintensity in T2, often coupled with vasogenic oedema.6 The mesothelioma metastasis in our case demonstrated distinctive MRI appearances not commonly seen in other CNS metastases. Our case demonstrated a ring-enhancing lesion, which had a homogenously enhancing and uniformly thickened circumference, with high cellularity and centrally necrotic core. The presence of a highly thickened ring around a centrally necrotic core is an unusual and striking radiological feature and was thus called the ‘donut sign’. In our review of the literature, we identified four patients from other case reports with available imaging, of which three had similar features resembling the ‘donut sign’ as we have described.1 3 5 While the underlying pathological mechanism for this unique radiological appearance is unknown, we hypothesise it may be related to a pathophysiological predisposition to laying down greater amounts of connective tissue within the developing tumour capsule. The exact significance of this radiological appearance is yet unknown; however, with further reporting in the literature and an appreciation for this provided description, a clearer understanding may emerge.
Furthermore, the current autopsy series of patients with mesothelioma suggest CNS diseases may be an under-reported phenomenon. In one systematic review of the literature, evidence of CNS metastases was found in 2.7% of cases of malignant mesothelioma.1 This systematic review included a pooled analysis of 7 autopsy series and identified 655 cases. This indicates that metastases to the brain may occur more commonly than we currently appreciate. The under-reporting may relate to a lack of symptomatology within the limited lifespan of the patients.
In conclusion, our case highlights a rarely encountered clinical entity of cerebral mesothelioma metastasis. Our case adds to a limited body of evidence to help detail the behaviour of mesothelioma CNS metastasis. These lesions may have a unique appearance on MRI termed ‘donut sign’. Furthermore, autopsy series indicate this disease may be under-reported and thus emphasise the importance of such case reports that may outline the clinical course and underlying pathological findings.
Patient’s perspective
It all started 2–3 days before I came into hospital. My wife was out one time, and I decided to go out onto my stationary bike to do some exercise. I walked downstairs to get on the bike, and I could only go for about 15 min before I came back upstairs. I could not find my back door key and began to feel very confused, so I tried to ring my wife. My wife came back home a few hours later and found me. Apparently, I was trying to speak to my wife, but it all came out sounding like gibberish. I thought I was speaking normally but no one could understand me. It wasn’t even scary to me at the time because I did not realise what was happening and didn’t realise I wasn’t making sense at the time.
When I got to hospital, I remember that the neurosurgery team spoke to me, and my wife says they explained everything to us. From my memory, I could not understand everything they were saying.
After the surgery I came out anaesthesia and one of the nurses asked me if I needed some Panadol for any head pain. But I had no pain at all. I said, “I’m not even having any headaches.” I thought it was unusual considering they had just operated on my head, but everything went smoothly. Overall, my experience in hospital was very good, I was amazed that after major surgery like that, that I was up and about. I really thought I would be flat on my back for weeks and weeks. It was frustrating after surgery because I still had some issues with words and my memory. I had to relearn almost everything…I couldn’t even figure out how to work the shower. But I was amazed that after a few days everything was coming back.
Now I can read and write but I still struggle when it comes to using a computer and I can never remember where the letters are. At night my wife writes and types for me because I get tired. I’ve regained most if not all my memory and although I’m not fully back to my hobbies. I’m still able to ride my bike 2–3 times a week. I still have breathlessness because I’m undergoing immunotherapy and chemotherapy which has affected my lungs. But I don’t feel any issues with my brain. I have setbacks now and again but they’re due to my lung cancer not my brain. I think my memory has improved as far as it can which is good.
Learning points
Malignant mesothelioma may metastasise to the brain despite the low reported rates in the literature.
Mesothelioma central nervous system (CNS) metastasis may have a unique radiological appearance termed ‘donut sign’.
Autopsy series suggest that mesothelioma CNS metastases may be under-reported in the clinical setting.
Ethics statements
Patient consent for publication
Acknowledgments
Westmead Hospital Neurosurgery Department and Westmead Hospital Pathology Department.
Footnotes
Contributors OA contributed by acquiring the patient’s electronic medical records, surgical notes and pathology reports to draft the body of the manuscript and contributed to the literature review required for the background portion of the manuscript. YL was responsible for conception and design of the case report as well as final approval of version submitted. AD was involved in editing drafts of the manuscript and literature review necessary for the development of the discussion.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.