Article Text

Abstract
A 59-year-old woman underwent an open pancreaticoduodenectomy. Thoracic patient controlled-epidural anaesthesia provided excellent incisional pain relief; however, the patient experienced intractable left shoulder pain (10/10 on the Numerical Rating Scale). To our knowledge, there is no effective established treatment for patients experiencing shoulder pain after an open pancreaticoduodenectomy. The patient’s shoulder pain did not respond to medical management with acetaminophen, ketorolac, lidocaine transdermal patch, oxycodone and hydromorphone. Then, on postoperative day 2, the acute pain service was consulted. Considering that the sphenopalatine ganglion block has been previously reported to be helpful in a number of painful conditions, including shoulder tip pain after thoracic surgery, we offered this treatment to the patient. After just one topical sphenopalatine ganglion block, using a cotton-tipped applicator, the patient’s shoulder pain entirely resolved and did not return. This is the first report of a successful treatment of intractable ipsilateral shoulder pain following an open pancreaticoduodenectomy with transnasal sphenopalatine ganglion block.
- pain
- gastrointestinal surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Pancreaticoduodenectomy (aka Whipple procedure) is one of the most complex surgeries and is often associated with a high rate of major complications and severe postoperative pain.1 Incisional abdominal pain after pancreaticoduodenectomy can be well controlled with epidural techniques and additional intravenous opioids. Although significantly more common in patients who undergo laparoscopic surgeries, some patients who undergo open procedures may experience postoperative ipsilateral shoulder pain. This type of pain is caused by the irritation of tissues supplied by the phrenic nerve. To treat shoulder tip pain, which is precipitated by diaphragmatic irritation, the C3, C4 and C5 nerve roots must be blocked, but as this would inhibit phrenic nerve function and cause apnoea, it is not an option. Furthermore, this type of pain is often not responsive to systemic analgesics, such as non-steroidal anti-inflammatory drugs and opioids.2
To our knowledge, there is no effective established treatment for patients experiencing shoulder pain after an open pancreaticoduodenectomy. Sphenopalatine ganglion block (SPGB) was first reported as a treatment for unilateral facial pain symptom complex in 1908 and has since then been used to treat a number of painful conditions.3 This is the first report of a successful treatment of intractable ipsilateral shoulder pain after an open pancreaticoduodenectomy with topical transnasal SPGB using a cotton-tipped applicator. Written informed consent was obtained from the patient for publication of this report.
Case presentation
A 59-year-old woman with a prior medical history of hypertension, hyperlipidemia and intraductal papillary mucinous neoplasm of the pancreas underwent an open pancreaticoduodenectomy, portal lymphadenectomy, retroperitoneal lymphadenectomy and pancreatic ultrasound. The surgery was performed under general and thoracic epidural anaesthesia (catheter inserted at T7–T8 level). There were no intraoperative complications. Postoperative pain was managed using patient controlled-epidural anaesthesia (PCEA) with bupivacaine 0.1% with 2 µg/mL fentanyl with a basal infusion of 8 mL/hour and a 2 mL PCEA dose with a lockout of 12 min. The epidural PCEA provided excellent incisional pain relief; however, the patient experienced left shoulder pain (Numerical Rating Scale (NRS) 10/10 for most of the day) that did not respond to acetaminophen 975 mg PO every 6 hours, ketorolac 15 mg IV every 8 hours, lidocaine 5% transdermal patch, hydromorphone 0.5 mg every 4 hours, oxycodone 5 mg PO every 4 hours and oxycodone 10 mg PO every 4 hours.
Investigations
On postoperative day 2, the acute pain service was consulted to evaluate the patient’s shoulder pain. The patient reported that she had a remote history of left shoulder pain 10 years prior to admission that resolved with physical therapy and intra-articular steroid injections. She reported that the postsurgical pain she was currently experiencing in her left shoulder was ‘excruciating’ and that it was significantly different from the type of pain she had 10 years ago. She described her current pain as sharp and needle-like sensation inside her shoulder that would randomly get significantly worse throughout the day since the surgery. The pain, when it was at its worst, would last in severity for 30 min.
Differential diagnosis
The differential diagnoses included pain from surgical positioning, immediate postoperative complications, such as anastomotic leak or subphrenic collections, cardiac complications, pulmonary complications and/or referred pain from manipulation of the pancreas. The patient was afebrile and had no leukocytosis. Chest X-ray findings included: heart and mediastinum of normal size and contour; linear opacity in the left lower lobe likely representing atelectasis; no developing chronic heart failure or pneumonia; osseous structures unremarkable, particularly involving the left shoulder; no acute fracture or dislocation; and unremarkable acromioclavicular joint. This suggested that the source of the pain was not from surgical malposition nor from a pulmonary complication. ECG showed sinus rhythm, heart rate of 79 beats per minute with normal axis, which made the shoulder pain from a cardiac complication less likely. Since there were no signs of systemic infection at that time, which could point towards immediate postoperative complications, the primary surgical team chose not to do a CT scan at this time. The remaining differential diagnosis was referred pain from manipulation of the pancreas.
Treatment
Based on a recent publication of the SPGB being an effective treatment for post-thoracic shoulder tip pain4 and our observation of the block being an effective treatment for various headache and neck pain aetiologies in our pain clinic, we offered the SPGB to this patient. On discussion of potential risks and benefits of the procedure, including the option of not proceeding, the patient elected to go ahead and signed a written informed consent.
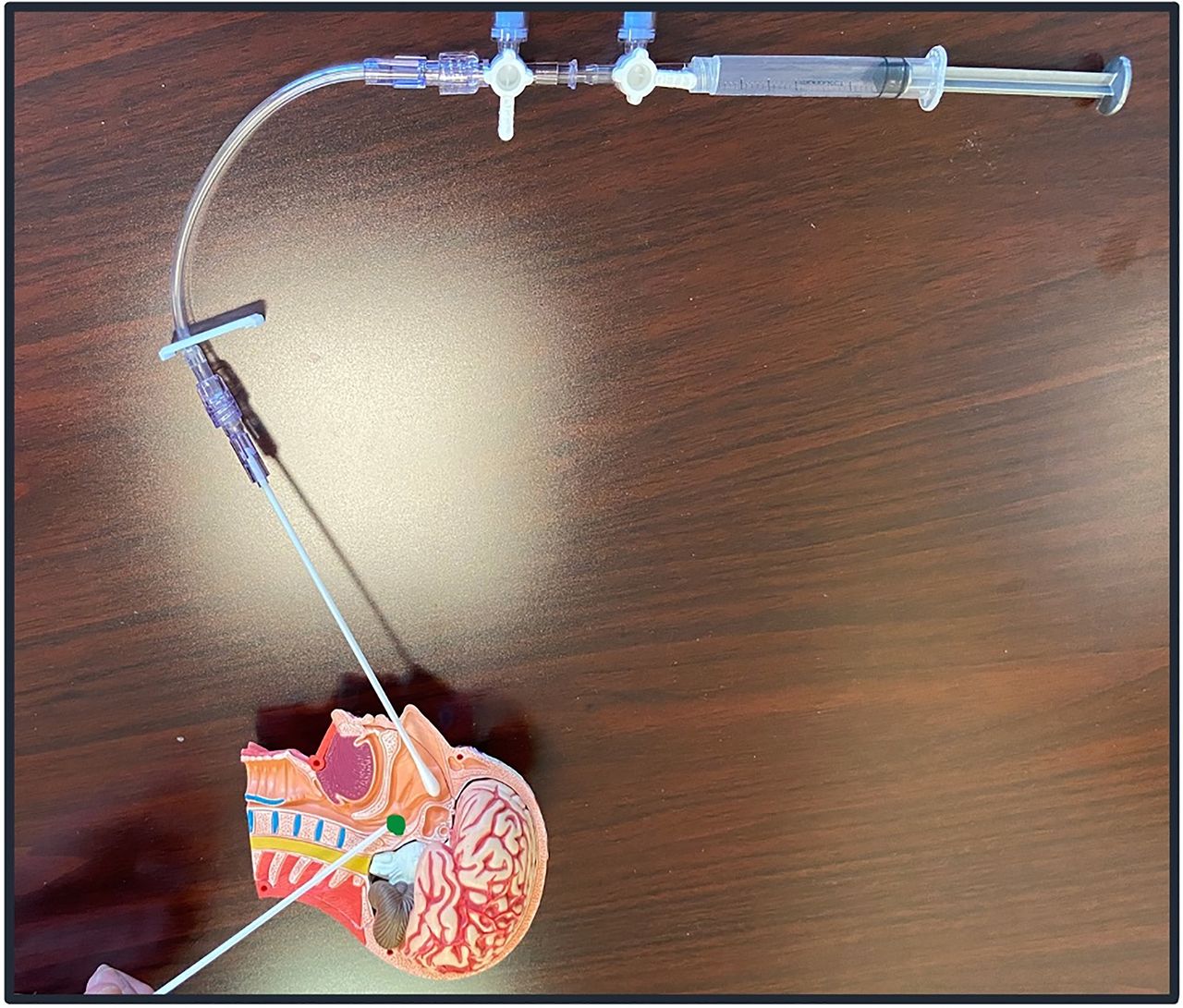
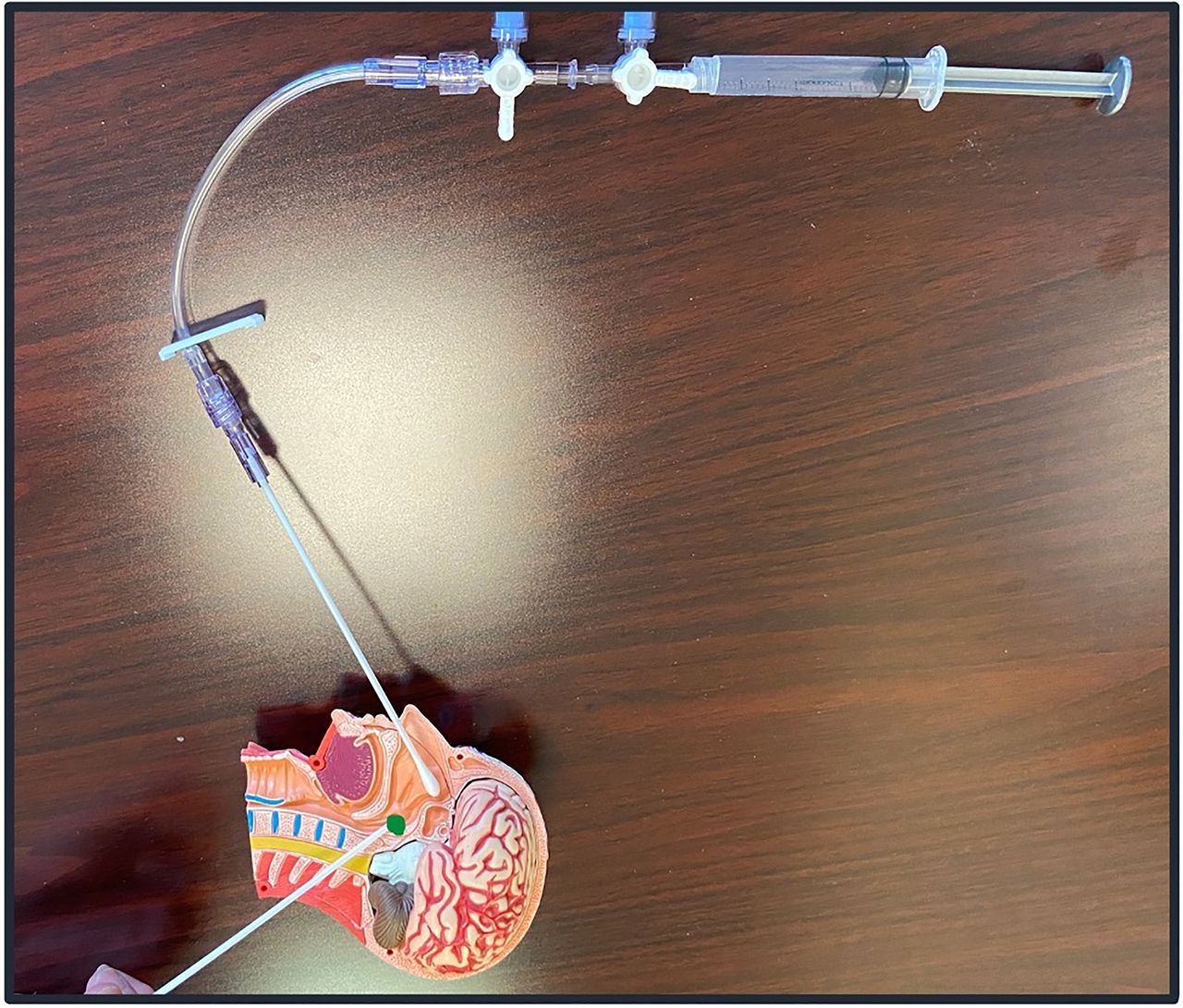
At the start of the procedure the patient’s left shoulder pain was 5/10 on the NRS. SPGB applicators were created from hollow cotton swabs, intravenous extension tubing with a stop cock, 3 mL syringes, 5% lidocaine ointment and 4% lidocaine topical solution (figure 1). The patient was positioned in the supine position with her head off the bed, supported by a pillow, for cervical spine extension (chin-up position) (figure 2). Haemodynamic monitors consisting of non-invasive blood pressure, pulse oximetry and EKG were applied, and the patient remained haemodynamically stable throughout the procedure. The SPGB applicator dipped into lidocaine ointment was gently inserted into each nostril atraumatically and stopped at the point where gentle resistance gave way at the junction of the turbinates and aperture of the nasopharynx. Lidocaine 4% was dripped drop by drop through the applicators into each nostril until the patient felt the medication in the back of her throat (1 mL into the right nostril and 0.5 mL into the left nostril) (figure 3). The SPGB applicators were left in place for a total of 15 min while the patient had a small towel covering her eyes for comfort.

Creation of the sphenopalatine ganglion block (SPGB) applicator: Supplies (lidocaine 4% topical solution, lidocaine 5% ointment, scissors, hollow cotton-tips, 3 cc syringes, Anaesthesia IV Set and towel to cover eyes (optional)); Disconnect the ‘Anaesthesia IV Set’ and cut the purple tip with scissors; Disconnect the tip of the ‘Anaesthesia IV Set’ and toss the tip; Connect all the remaining pieces together.

The positioning of the sphenopalatine ganglion block (SPGB) applicators in a mannequin model.
{kind=link}
{kind=link}
{kind=link}
The sphenopalatine ganglion block (SPGB) applicator on a mannequin model demonstrating that once a patient feels the medication in the back of the throat, the medication has reached the SPGB (marked with the green circle).
Outcome and follow-up
At the end of the procedure, the patient was asked to sit up. She reported that her shoulder pain had entirely resolved, 0/10 on NRS.
During the procedure, the patient reported having some difficulty swallowing because it felt like the back of her throat was numb. This sensation resolves on its own after several minutes. On postoperative day 12, when the patient was being discharged from the hospital, she remained pain free in her shoulder. The patient was followed up 1 month later via a telephone call. At that time, the patient excitedly reported that she has been pain free in her shoulder since the SPGB treatment.
Discussion
Open pancreaticoduodenectomy is one of the most complicated surgeries and involves a significant amount of intra-abdominal manipulation. When the head of the pancreas is affected, patients typically perceive pain in the T5–T9 regions; however, when the tail of the pancreas is involved, patients experience referred pain to the left shoulder secondary to the innervation of the C3–C5 dermatomes.5 6 As in our patient’s situation described above and in many other pancreaticoduodenectomy surgeries, when the epidural is inserted at the thoracic level, the epidural is unable to relieve a patient of the referred shoulder pain. Systemic medications, such as non-steroidal anti-inflammatory drugs and opioids, are often trialled with limited effectiveness.2 Furthermore, opioids are commonly associated with adverse reactions, such as respiratory depression, sedation, dizziness, gastrointestinal disturbances, tolerance and physical dependence.7
When the administration of acetaminophen, ketorolac, lidocaine transdermal patch, oxycodone and hydromorphone did not provide sufficient left shoulder pain relief to our patient, the SPGB, a technique first described by Sluder over a century ago,8 was used and found to be highly effective. The precise neurophysiological mechanism that explains the observed results in our patient is unknown; perhaps it will be elucidated with future work.
Since there is only one sphenopalatine ganglion, the commonly accepted SPGB technique is to place local anaesthetic topically by way of both the left and right nasal passages local anesthetic-soaked swabs, contributing to successful transmucosal reach and coverage of the SPG.9 However, the sphenopalatine ganglion is a bilateral structure, so, in theory, a block just through the left nasal passage could have also potentially achieved the observed result. There are several commercially available devices available to perform SPGB, but the administration of this block via the assembly of cotton-tip applicators from supplies that are readily available in most medical centres is simple and inexpensive.4 9–13 The fascinating aspect of this block is that not only does it treat numerous pain conditions, including headaches of various aetiologies, neck pain, back pain6 10–13 and now postoperative shoulder pain, but it also, somehow, has a long-term effect. Even after the temporary effects of local anaesthetic wear off, certain pain conditions resolve and never return after this treatment. This interesting phenomenon would benefit from further investigation. In the meantime, we suggest that this technique be considered for patients with postsurgical shoulder tip pain.
Learning points
This is the first report of a successful treatment of intractable ipsilateral shoulder pain after an open pancreaticoduodenectomy with topical transnasal sphenopalatine ganglion block using a cotton-tipped applicator.
Although there are several commercially available devices available to perform sphenopalatine ganglion blocks, the sphenopalatine ganglion block can also be effectively performed by quickly and inexpensively creating cotton-tip applicators from supplies that are readily available in most medical centres.
The cotton-tip applicators can be created from the combination of hollow cotton swabs, intravenous extension tubing with a stop cock, 3 mL syringes, 5% lidocaine ointment and 4% lidocaine topical solution.
Ethics statements
Patient consent for publication
Footnotes
Twitter @daniellelevinmd
Contributors DL, MA, JC, and FG contributed to the concept, design, data collection/processing, analysis/interpretation, literature search, writing manuscript and critical review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.