Article Text

Abstract
Sarcoidosis is a multisystem inflammatory disorder of uncertain aetiology. There are numerous case reports of sarcoidosis occurring during treatment with biological immunotherapies. Here, we describe the case of a 52-year-old woman with psoriatic arthritis who developed multisystem sarcoidosis while being treated with secukinumab (anti-interleukin-17A) therapy which, to our knowledge, is the first such case. We discuss existing literature and hypothesise that IL-17 blockade may precipitate the development of granulomatous disease.
- drugs: musculoskeletal and joint diseases
- biological agents
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Sarcoidosis is a multisystem disorder characterised by the presence of non-caseating granulomata. While the disease is most commonly characterised by thoracic adenopathy, lung parenchyma, skin and articular disease, all organ systems may be affected. While the precise aetiology of sarcoidosis is unclear, numerous case reports of sarcoidosis occurring during the treatment with biological immunotherapies indicate that immune dysregulation plays a key role. Here, we describe a case of sarcoidosis developing following treatment with anti-interleukin-17A therapy (anti-IL-17A), which to our knowledge is the first such case.
Case presentation
A 52-year-old woman was referred to rheumatology outpatient clinic with new widespread peripheral joint and left buttock arthralgia and generalisation of palmoplantar psoriasis despite treatment with subcutaneous methotrexate 20 mg and folic acid 5 mg by mouth weekly.
Medical history was significant for an acute hospital admission 2 years previously with shortness of breath. CT pulmonary angiogram at that time revealed segmental collapse secondary to mucus plugging with no other abnormalities. Our patient was treated for asthma with long-acting beta agonist and corticosteroid inhalers.
Clinical examination revealed asymmetric synovitis of proximal interphalangeal (PIP), wrist and ankle joints (12 tender joints, 4 swollen joints), bilateral Achilles tendonitis with plantar fasciitis and marked tenderness of the left sacroiliac joint. A subtle degree of cutaneous plaque psoriasis was seen.
Investigations
Laboratory results showed a normal full blood count without oeosinophilia, elevated erythrocyte sedimentation rate (ESR) of 16 mm/hour (1–15), normal C-reactive protein (CRP) and normal rheumatoid factor, anti-cyclic citrullinated peptide (anti-CCP) and anti-neutrophil cytoplasm antibody titres. Plain radiographs of hands, feet and chest at this time were unremarkable and a diagnosis of active psoriatic arthritis was made.
Differential diagnosis
Our patient had a prior diagnosis of psoriasis, had active skin lesions and had an asymmetric oligoarthritis typical of psoriatic arthritis. Prior treatment with tumour necrosis factor-alpha inhibitor (TNFi) therapy and hilar adenopathy on CT raised the suspicion of both lymphoma and Mycobacterium tuberculosis infection. However, no B-symptoms were reported, serum lactate dehydrogenase (LDH) was within normal limits, interferon-gamma-release-assay was negative, hilar lymph node biopsies showed no evidence of malignancy and mycobacterial cultures from lymph node tissue were negative.
Treatment
After failed responses to sequential treatment with methotrexate 25 mg weekly in combination with sulphasalazine 1000 mg by mouth two times per day, followed by the TNFi adalimumab 40 mg s.c. (subcutaneous) fortnightly, articular and cutaneous remission was achieved with secukinumab 300 mg s.c. monotherapy weekly for 5 weeks, followed by once monthly.
Outcome and follow-up
Six months following secukinumab commencement, our patient represented with a new dry cough, exertional dyspnoea and recurrent polyarthralgia. Clinical examination and bedside ultrasound revealed finger dactylitis (figure 1A), bilateral knee synovitis and left-sided posterior tibialis tenosynovitis (figure 1B). A widespread violaceous rash affecting the eyelids, trunk and limbs was seen.

(A) Palmar longitudinal view of dactylitic finger showing tendon sheath effusion with power Doppler signal. (B) longitudinal view of posterior tibialis tendon showing tendon sheath effusion, tenosynovial thickening and power Doppler signal.
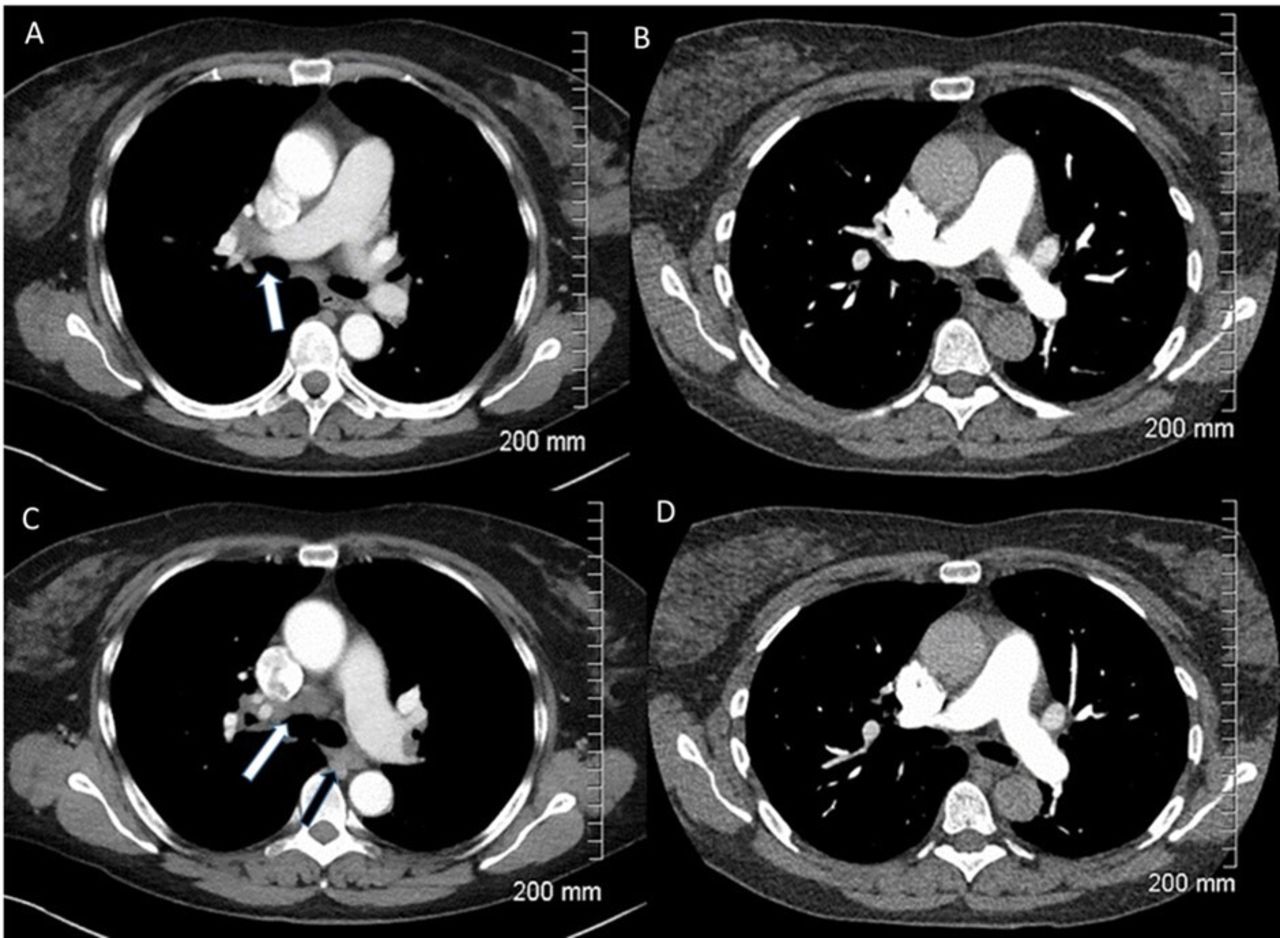
Laboratory markers showed elevated ESR (40 mm/hour) and CRP (20 mg/L). Chest X-ray was suggestive of lung nodularity with hilar enlargement and CT thorax demonstrated parenchymal solid and ground glass nodules with hilar and paratracheal lymphadenopathy (figure 2). Serum ACE (angiotensin-converting enzyme) and LDH were within normal limits and interferon-gamma-release-assay was negative. Pulmonary function tests (PFTs) showed a mild restrictive defect with transfer factor for carbon monoxide (TLCO) 80% predicted. Endobronchial ultrasound with biopsy of an affected lymph node and cutaneous biopsies confirmed the presence of non-necrotising granulomata (figures 3–4).
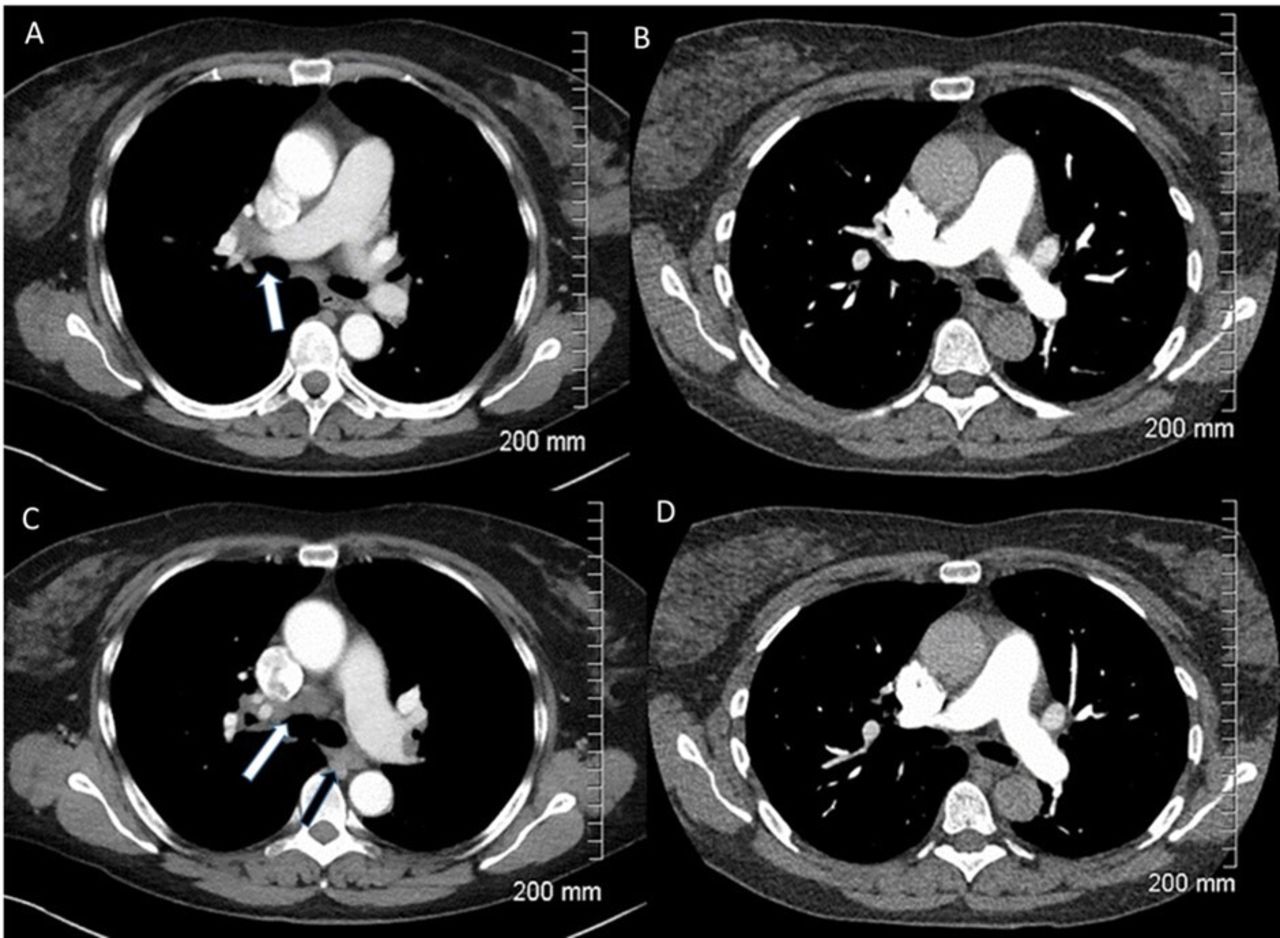
(A) Axial postcontrast CT image, soft tissue window, showing right hilar adenopathy (arrow). (B) CTPA from 2 years previously showing no adenopathy at that time. (C) Axial postcontrast CT image, soft tissue window, showing right lower paratracheal (white arrow) and left lower paratracheal (black arrow) adenopathy. (D) Comparative CTPA from 2 years previously showing no adenopathy at that time. CTPA, CT pulmonary angiogram.

Sarcoid at ×4. Dermis expanded by multiple non-caseating granulomata (white arrow), with foreign body giant cells (black arrows). No foreign material, micro-organism stains negative.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sarcoid at ×20. Non-caseating granulomata (white arrow) with lymphocytic cuff (black arrow).
A diagnosis of multisystem sarcoidosis was made and prompt induction of remission was achieved using prednisolone 30 mg by mouth daily. Remission was maintained at a recent 3-month follow-up review at which point our patient was taking prednisolone 20 mg daily. This will be tapered by 5 mg monthly during regular follow-up and consideration will only be given to alternative biologic therapies in the event of a flare.
Discussion
In recent years, an increasing use of biological immunotherapies for autoimmune diseases has been associated with sporadic case reports of de novo sarcoidosis or exacerbations of pre-existing disease. While most frequently associated with TNFi, this phenomenon has also been observed following treatments that inhibit interleukin 2 (IL-2), IL-6, IL-12/23, IgE, alpha-integrin, cluster of differentiation 52 (CD-52), B-cells as well as with immune checkpoint inhibitors.1–11 Paradoxically, TNFi has also been used to treat various organ manifestations of sarcoidosis refractory to standard therapies indicating that a spectrum of immunopathology exists that requires future elucidation.12–15
Secukinumab is a human IgG1 monoclonal antibody that binds to the protein interleukin-17A. While there are no previous reports of sarcoidosis developing during treatment with secukinumab to our knowledge, treatment with IL-17A inhibition has been associated with the development, and exacerbation, of disease activity in other granulomatous diseases such as Crohn’s disease.16 Formation of sarcoid granulomas is thought to begin with foreign antigen presentation to CD4 +T helper lymphocytes which then stimulate the immune response via interferon-gamma, IL-2, TNF alpha and multiple other cytokines.17–22 The potential role for IL-17A in sarcoid pathogenesis has been suggested by the finding of increased IL-17A levels in bronchoalveolar lavage (BAL) fluid obtained from sarcoidosis patients while a case report showed significant improvement in a patient with TNFi-induced pulmonary sarcoidosis following anti-IL-17A therapy.23 24
The apparent association observed between IL-17 inhibition and granulomatous diseases such as Crohns, and now sarcoidosis, suggesting a common underlaying mechanism. Further understanding of this mechanism as well as understanding the apparent paradoxical effects observed with IL-17i in sarcoidosis is required to direct future individualised approaches to treatment of this complex multisystem inflammatory disease. Our case also highlights the importance for rheumatologists to continually monitor for de novo activation of other disease states, and indeed unforeseen reactivation of dormant disease states, in those with pre-existing inflammatory disease.
Patient’s perspective
Since this all started, I have lost my life as I knew it. I was an older woman but I was running, attending 3–4 gym classes per week, hill walking, playing golf, living life to the full and enjoying a social life too. I had met my now husband, and we had set up home together, after which I began to get sick.
I developed a rash on my buttocks and legs, then on my hands and feet and my dermatologist diagnosed psoriasis. My sister organised for me to see another dermatologist, who when I was there had checked my joints and said they were all inflamed. I was feeling pretty miserable and my feet were so painful to walk on. PUVA didn’t work and Methotrexate only worked for my skin, not my joints. A rheumatologist then diagnosed me with psoriatic arthritis and started me on adalimumab. At this point I could barley walk, my life had completely changed but I was trying to get on with it as I had recently got married. I had little or no response to the adalimumab so the rheumatologist put me on Secukinumab and this was a big change for me.
All of my joints began to ease within a couple of weeks and this felt like a new lease of life, I was feeling so well. I had taken back up my golf and it was great to be out in the air and feeling like I was in the land of the living. I was doing a spinning class as this was easier on my joints. I really thought “this is it”.
After my symptoms flared again, I was also diagnosed with sarcoidosis. When I think about it now, it was just another thing. But getting a diagnosis felt great, like ‘I know what I have now maybe they can start to treat everything that’s going on with me’. I was disappointed that I had to stop Secukinumab as this was the only thing that seemed to be working.
Of course there were frustrations, having to have different treatments but also there was hope that with each one this would be the one that worked, that gave me back my life. I was told I have both sarcoidosis and psoriasis, but to be honest all I was looking for was what treatment and what impact will this have on my life now, as I felt like I can’t do much more of this.
My rheumatologist admitted me to hospital for some tests. I had a biopsy on my arm and some scans. I was then told it was in my lungs and had an Endobronchial Ultrasound. I was started on 30 mg of steroids which have driven me quite mad I have to say. I’m up working (from home) between 3.00am and 4.00am. Most of my joints have freed up and I am beginning to feel a little more normal. As the steroids reduce, I am beginning to see and feel the benefits of them. I now have more energy and my brain doesn’t seem to be in a constant fog. All I hope is that it works. I’ve become quite anxious but of course that also is the medication. I am trying to keep my job going (I have a very understanding boss) and as for the rest of my life, I feel that its on hold.
This has taken me nearly 3 hours to write as I hadn’t realised how much this has affected my life. In the last few years, I have been just plodding along hoping that something would work. I have learnt that I am quite a strong person internally but something tells me if I shouted louder earlier maybe things would have been different. I’m still very hopeful that this will work.
Learning points
This is the first case reported of sarcoidosis manifesting during the treatment with secukinumab (anti-interleukin-17A, IL-17Ai).
IL-17Ai has been associated with the development of Crohn’s disease, suggesting a common underlaying mechanism between IL-17Ai and the development of granulomatous disease.
The paradoxical effects observed with IL-17i and sarcoidosis indicates that a spectrum of immunopathology exists that requires future elucidation to direct future individualised treatment approaches.
Our case highlights the importance for rheumatologists to continually monitor for de novo activation/reactivation of other disease states in those with pre-existing inflammatory disease.
References
Footnotes
Twitter @ckirb19
Contributors All listed authors contributed to this work. CK and RM were both involved in the clinical care of the patient and in acquiring ultrasound images. DH evaluated the radiological images and LC analysed biopsy specimens.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.