Article Text

Statistics from Altmetric.com
Description
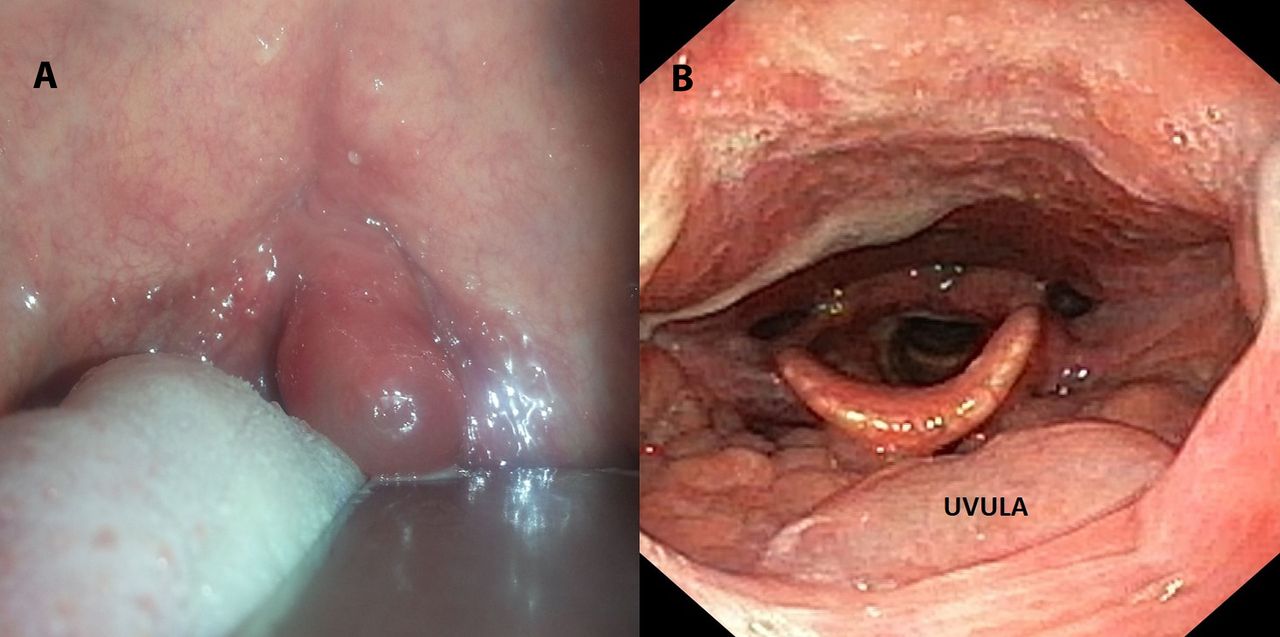
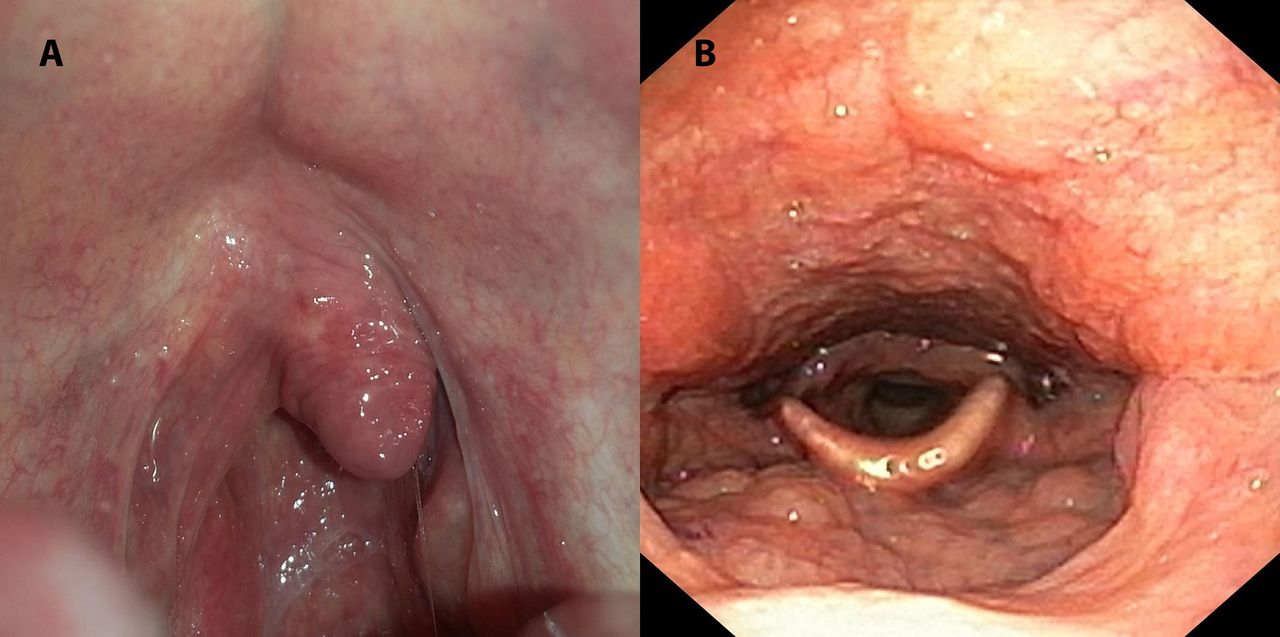
A 32-year-old man presented to the otorhinolaryngology emergency with complaints of sudden onset of foreign body sensation in his throat associated with drooling and muffled voice. The patient had consumed seafood (prawns) the previous night and woke up with the sensation of something ‘stuck’ in the back of his throat. Patient denied any pain, fever, trauma or past history of food/drug allergy. Physical examination revealed an enlarged, swollen and congested uvula touching the base of tongue (figure 1). Rest of the examination was unremarkable and his vitals were normal. A clinical diagnosis of Quincke’s disease was made possibly due to an allergic reaction to the seafood. He was treated with a single dose Inj. dexamethasone (8 mg), Inj. chlorpheniramine maleate (25 mg) and epinephrine nebulisation. About 2 hours later, uvular oedema completely disappeared along with resolution of symptoms (figure 2). The patient was discharged on oral antihistamines and was advised to avoid seafood. At 6 months follow-up, the patient remained symptom free.
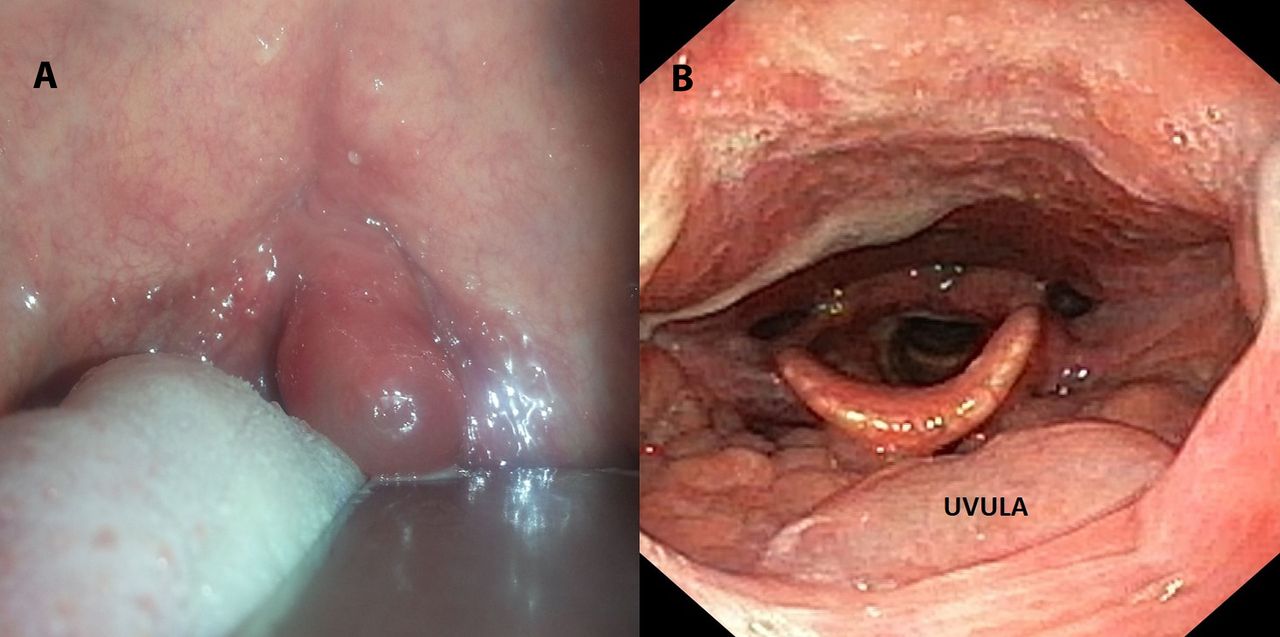
Clinical image depicting gross oedema of the uvula, touching the base of tongue.

{kind=link}
{kind=link}
Clinical image showing complete resolution of uvular oedema 2 hours after treatment.
Isolated uvular angioedema or Quincke’s disease is a rare presentation of angioneurotic oedema affecting only the upper airway. Various etiological factors like food allergy, hereditary angioedema, inhalation exposure, drug reactions and trauma have been implicated.1 2 Peanuts, tree nuts, fish and shellfish account for the vast majority of severe food anaphylactic reactions.1 The most common underlying aetiology is type I immediate hypersensitivity reaction, seen with atopic states and specific allergies.2 Recurrent attacks are observed in disorders of compliment system like hereditary angioedema and acquired C1 esterase inhibitor deficiency.3 This condition can compromise the airway rapidly and lead to potentially a life-threatening situation. Hence, initial management should be focused on restoring and assuring a safe airway. The medical treatment consists of intravenous H1 and H2 histamine blockers, parenteral and inhalational corticosteroids, beta-2 mimetics like albuterol or salbutamol and nebulised or topical epinephrine.1 3 4 However, parenteral epinephrine should be considered in severe cases. Dexamethasone, because of its potent anti-inflammatory properties and long half-life, is considered the corticosteroid of choice.4 Observation is mandatory following an acute phase to assure that no further swelling occurs. Patient can then be discharged on oral antihistamines and tapering course of steroids.2 5 Quincke’s disease should be differentiated from infectious uvulitis, which is generally associated with tonsillitis, pharyngitis and epiglottitis, causing pain and fever. This distinction is important due to therapeutic implication, as the latter needs antibiotic therapy.
Patient’s perspective
Sunday morning I woke up with feeling of something stuck in my throat and change in my voice. Whenever I try to swallow there was excessive gag and vomiting sensation. I had no such previous episodes and I rushed to the hospital emergency. On examining, doctors informed me that I am having a swelling in my throat due to some allergy and they added its emergency to get admitted. I was really worried about my condition. To my surprise, with single dose of injection, I started feeling greatly relieved and within 2 hours, I was back to normal. The doctors said my condition was Quincke’s disease and probably triggered by the seafood (prawn) which I had consumed the evening before. They kept me on observation till evening and came home back happily.
Learning points
Quincke’s disease usually presents with a foreign body sensation in the throat in a previously well patient. Fever and pain are frequently absent.
The uvula is oedematous and it can compromise the airway rapidly and lead to potentially a life-threatening situation so assurance of a patent airway is of paramount importance.
The medical treatment consists antihistamines, parenteral or inhalational corticosteroids, beta-2 mimetic and rarely epinephrine.
Footnotes
Contributors AC has conceptualised the article and PS had made changes and modifications with ASC finalising the paper. All three were involved in the clinical care of the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.