Article Text

Abstract
Neuroendocrine neoplasms (NENs) are malignancies with rare reports of central nervous system development. A 34-year-old woman was found to have a primary NEN of the brain, and she had recurrence with identical histology 10 years later. Extracranial NENs were excluded. She had routine surveillance for the first 5 years with MRIs and positron emission tomography/CTs after the initial presentation which was treated with radiation followed by cisplatin and etoposide. This case highlights the difference in primary NENs versus NEN metastases to the brain, and that longer periods of surveillance are likely required for primary NENs. This is important because the prognosis between primary NENs and metastatic NENs to the brain are vastly different and should not be treated as equal diseases. The patient eventually died of her recurrence secondary to complications of a ventriculoperitoneal shunt placed for treatment of hydrocephalus from the disease.
- neurooncology
- neuroendocrinology
- CNS Cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
The neuroendocrine system comprises a complex architecture of cells that are capable of producing neuroendocrine neoplasms (NENs) throughout the body. These cells are found diffusely throughout different organs and are well described throughout the gastrointestinal tract, the respiratory tract and within the central nervous system (CNS).1 2 While NENs are known to develop in all of the aforementioned systems, there are only few reports to suggest NENs originating primarily from the brain. Neuroendocrine cells are naturally involved in the coordination of neurotransmitter-initiated synthesis and release of biologically active substances. Therefore, NENs possess unique properties such as secreting physiologically active amines and peptidyl hormones which allow NENs to retain unique methods for identification.1 3
The incidence of NENs has been prominently increasing over the past two decades.4 This is believed to be secondary to increased detection rates.2 While the incidence is increasing, these tumours are still very uncommon, and they account for only 4%–6% of all extracranial malignancies.5 NENs most commonly arise from the lungs, liver and the gastrointestinal tract.2
In rare instances, NENs can metastasize to the CNS. The incidence of patients with NENs having brain metastases is <5%. Furthermore, only 1.4% of metastatic brain tumours are NENs, and the majority of these lesions originate from primaries in the lung.6 When patients do present with metastatic NENs to the brain, they typically present with other local and distant metastases.6
Often, when NENs of the brain are discovered as the first sign of disease, an extracranial primary tumour is discovered on further diagnostic imaging.7 In cases when the extracranial NENs are diagnosed first, the time to brain metastasis is an average of 13 months. Brain metastases are associated with a poor prognosis, with a median overall survival of 8 months from the diagnosis of CNS involvement.7 However, the leading cause of death in patients with metastatic CNS NENs is secondary to systemic disease progression itself, with the majority of cases being associated with organ dysfunction (eg, liver failure).8
Here, we describe a case of a 34-year-old previously healthy woman who presented with symptoms of intracranial hypertension believed to be from a primary NEN of the brain. She was treated with adjuvant intensity-modulated radiation therapy (IMRT) followed by four cycles of cisplatin and etoposide and had locoregional reoccurrence of the primary NEN in the same area a decade later (see figures 1–3). No other sources of a primary tumour were ever discovered despite immense diagnostic testing.

T2 FLAIR sequence MRI of the reoccurrence near the right thalamus.
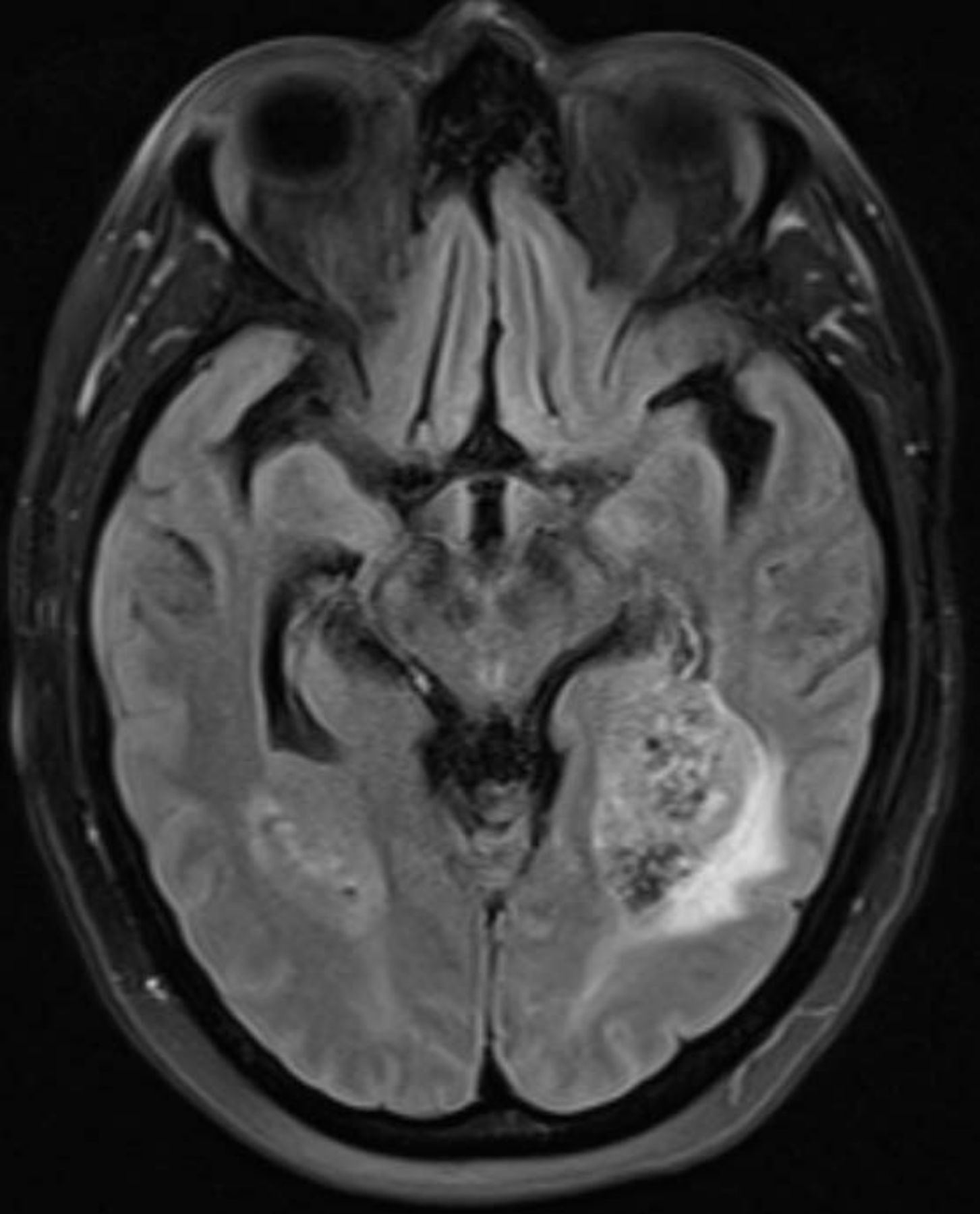
T2 FLAIR sequence MRI of the bilateral haemorrhagic masses which reoccurred in the ventricular atria.

T2 FLAIR sequence MRI showing a reoccurrence near the right ventricle.
Case presentation
A 34-year-old woman with no significant past medical history presented with worsening headaches, nausea and emesis. An MRI of the brain demonstrated a singular 1.5 cm lesion in the third ventricle near the foramen of Monro. She subsequently underwent superior right frontal craniotomy with resection of the anterior, superior third ventricular mass. Initially, the tumour was described as a neuroblastoma, but referral to a specialised pathology lab described it was more consistent with an NEN. The tissue was strongly positive for synaptophysin and chromogranin, and neurofilament staining was focally positive (see figure 4). Epithelial membrane antigen (EMA), glial fibrillar acidic protein (GFAP), neuronal nuclear antigen (NeuN), S-100, thyroid transcription factor-1 (TTF1), CDX2 and a pancreatic battery including insulin, gastrin, somatostatin, glucagon, vasoactive intestinal peptide (VIP) and pancreatic polypeptide (PP) were all negative, which favoured a neuroendocrine carcinoma over neuroblastoma.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
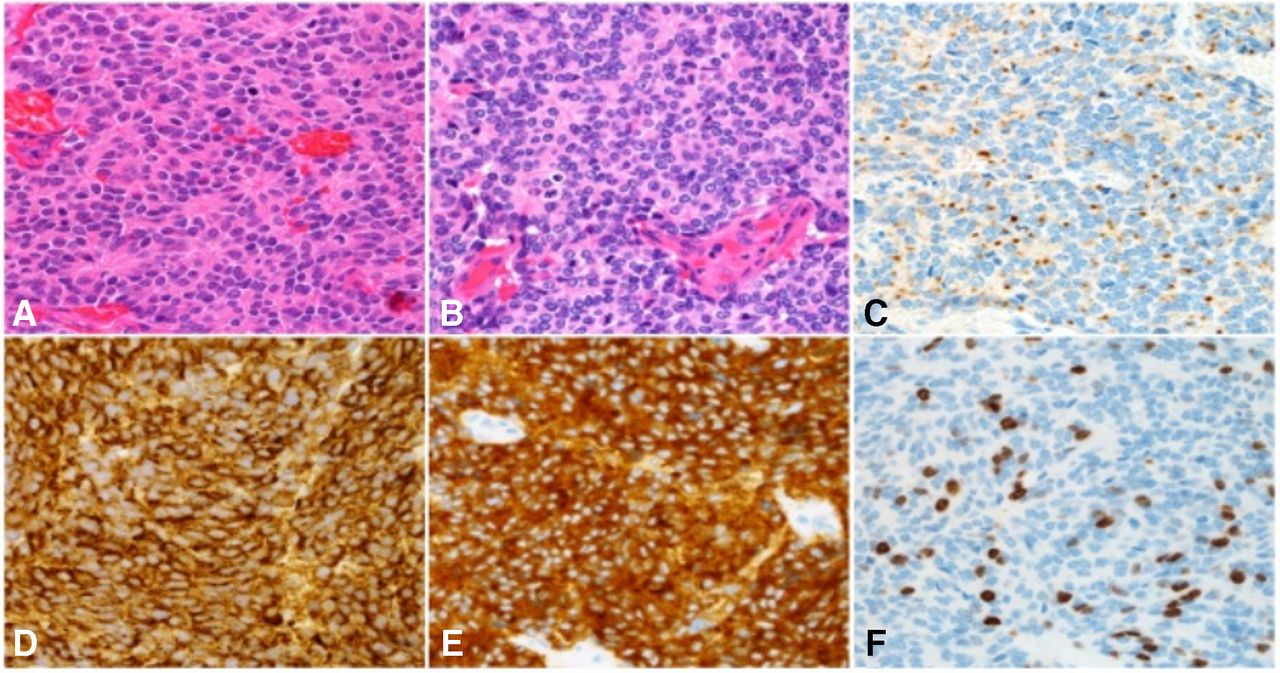
The tumour at first diagnosis (panel A, H&E section) and 10 years later (panel B, H&E section). The tumour is positive for cytokeratin CAM5.2 with a cytoplasmic dot-like pattern of stain typical of neuroendocrine tumours (panel C), chromogranin (panel D) and synaptophysin (panel E). Panel F shows the Ki-67 labelling (30%–35%).
A positron emission tomography (PET)/CT scan and an MRI of the complete spine were negative for any evidence of extracranial NEN. She underwent adjuvant IMRT with a total of 5400 cGy followed by four cycles of cisplatin and etoposide (doses, 75 mg/m2). After completion of therapy, the patient regained her baseline performance status of Eastern Cooperative Oncology Group performance status 0. She was followed with scheduled brain MRIs and PET/CTs for 5 years without evidence of disease reoccurrence or primary extracranial NEN.
Ten years after the initial presentation, the patient presented with symptoms suggestive of increased intracranial pressure. She was experiencing nausea, vomiting and severe headaches worse in the supine position.
Investigations
An MRI of the brain revealed bilateral 3 cm masses in the ventricular atria and a smaller 1 cm right thalamic mass. She underwent resection of the right thalamic mass and final pathology demonstrated high-grade neuroendocrine carcinoma, with a Ki-67 of 30%–35%. This was identical to the sample collected a decade prior, and had the same histopathological testing as above. It was also negative for the pituitary transcription factors PIT1, SF1, GATA-3, INI-1 and SDH-B. CT images of the chest, abdomen and pelvis were negative for an extracranial NEN, and a complete spinal MRI was also negative.
Differential diagnosis
Initially, it was thought that she had a neuroblastoma, but the tissue was strongly positive for synaptophysin and chromogranin, and neurofilament staining was focally positive which suggested an NEN EMA, GFAP, NeuN, S-100, TTF1, CDX2 and a pancreatic battery including insulin, gastrin, somatostatin, glucagon, VIP and PP were all negative which helped rule out several other primary neoplasms of the brain and extracranial NENs.
Treatment
Postoperative care was complicated by hydrocephalus that required a ventriculoperitoneal (VP) shunt. Subsequently, the patient developed mild left hemiparesis and worsening mental status with a Glasgow Coma Scale of 14. The left-sided hemiparesis improved with physical therapy, and the decision was made to proceed with cisplatin and etoposide (doses, 75 mg/m2) due to prior favourable response to this therapy and a prolonged disease-free interval. Further radiation therapy was deferred until after chemotherapy with a goal of cytoreduction and smaller radiation volumes to reduce the risk of radiation necrosis or other toxicities.
Outcome and follow-up
After receiving the first cycle of chemotherapy in the hospital, she was discharged to her local oncologist. During the second cycle of chemotherapy, she had progressive complications with the VP shunt and ultimately passed away from complications related to elevated intracranial pressure 2 months after the recurrence.
Discussion
To our knowledge, our patient represents the first well substantiated report of an intraventricular primary NEN of the brain. Neuroendocrine cells are present in multiple organ systems, and primary NENs can develop in all of the systems where these cells have been described. The location of the initial primary lesion, within the third ventricle, may also hold significant importance. The paraventricular nucleus is a group of neuroendocrine cells located adjacent to the ventricles in the area of our patient’s NEN. While these typically are involved with the synthesis of posterior pituitary hormones, neoplastic transformation is possible.9
NENs can be categorised clinically as functional or nonfunctional depending on if increased hormone production is associated. Additionally, they can be categorised by anatomical location, and by their grade. Ki-67 is a function of the degree of proliferation because it is expressed in the actively dividing cells.10 Adequate classification of NENs allows clinicians to determine the best diagnostic modalities, treatment options and to better understand the disease prognosis.11 12
While a previous case suggests a possible primary CNS NEN in a 77-year-old woman, we believe a metastatic lesion would be more consistent with presentation described.13 An overall survival of 720 days and histology that was positive for TTF-1 suggests that this primary CNS NEN was of bronchopulmonary origin even though no extracranial primary was initially found.14 Furthermore, there are few other case reports of extra-axial primary NENs. These were described in the pineal gland, near the pituitary, and along the meninges.15–20
In the present study, there are several pieces of information that strengthen the suspicion that this was indeed a primary NEN of the brain. First, the location of the tumour is in a region of the brain with known neuroendocrine cells. The majority of metastatic disease most commonly occurs in areas of the brain at the gray–white junction.21 Second, the patient had a significantly long disease-free interval of 10 years, while the overall survival for patients with metastatic NEN to the brain is typically only 10 months.6 Third, the patient’s recurrence was locoregional within the ventricles. An extensive workup with CT and PET/CT imaging both at initial diagnosis and 10 years later at recurrence, were negative for extracranial disease. This strongly suggests that the brain was the primary and the only site of disease.
Because the leading cause of death in patients with brain NENs is secondary to systemic disease progression, the prognosis may be substantially different from metastatic brain NENs.8 Primary brain NENs appear to be more similar to non-metastatic NENs in which the 10-year overall survival rate is 47%.2
The standard imaging in the workup of NENs includes both CTs and FDG PET/CTs. The sensitivity of CT imaging for identification of a primary tumour in unknown primary NEN is 95%.22 When an NEN is of high grade, as in this case, FDG PET/CTs have excellent sensitivity in detecting them given their high metabolic rate. For example, a study found that 100% of biopsy-proven high-grade NENs were seen with PET/CTs.11 Our patient had multiple PET-CTs throughout her disease course that failed to find another primary location.
More information is needed on proper treatment of primary brain NENs. Current data suggest that in metastatic brain NENs, radiation therapy and surgery may be beneficial.8 Furthermore, platinum-based chemotherapy is suggested in high-grade NENs. In our case, our patient had a decade of remission with the adjuvant IMRT followed by cisplatin and etoposide. Thus, in primary NENs of the brain, this approach could be considered for treatment.
In metastatic brain NENs, it is suggested that MRIs of the head be obtained with increasing time intervals if disease-free images are obtained.12 However, this case suggests that lifelong annual MRIs may be the standard of care to detect reoccurrence, but the data regarding the duration of the surveillance are lacking.
Patient’s perspective
Her husband stated ‘It would be an honour of the family that my wife’s medical records could be used in helping others, she would have been pleased to know that she is still helping others in need’.
Learning points
The prognosis of a primary NEN is drastically different from metastatic brain NENs.
Extended surveillance may be needed due to risk of late recurrence (>5 years).
It is possible for patients with primary brain NENs to have an excellent response and have a high quality of life after treatment.
An acceptable treatment option for primary NENs of the brain is intensity-modulated radiation therapy followed by etoposide and cisplatin.
Acknowledgments
The authors would like to thank Dr Caterina Giannini from the Division of Anatomic Pathology and Department of Laboratory Medicine and Pathology and Dr Kenneth Merrell from the Division of Radiation Oncology for their helpful contributions to the case report.
References
Footnotes
Contributors CTR was the primary author of this paper and did the primary research and writing. ND helped with literature review and editing of the paper. TH and JB helped with guidance of current neuroendocrine tumour guidelines and helped review/edit the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Next of kin consent obtained.