Article Text

Statistics from Altmetric.com
Description
A 71-year-old woman with diabetes and hypertension came with complaints of incomplete recovery of vision post right eye cataract surgery performed 2 months prior to presentation. On examination, the best-corrected visual acuity in the right eye was 20/40 p, N6, and left eye was 20/50, N6. Her right eye examination showed prolapse of vitreous in the anterior chamber with incarceration in the inner lip of the superotemporal limbal incisional scar causing peaking of the pupil at 10 o’clock along with temporal decentration of the intraocular lens. There were multiple white dots with pigments seen in this vitreous framework (figure 1). On posterior segment examination, dense asteroid hyalosis (AH) was observed with a hazy view to the underlying disc and retina. Her left eye was unremarkable except for nuclear sclerosis cataract.
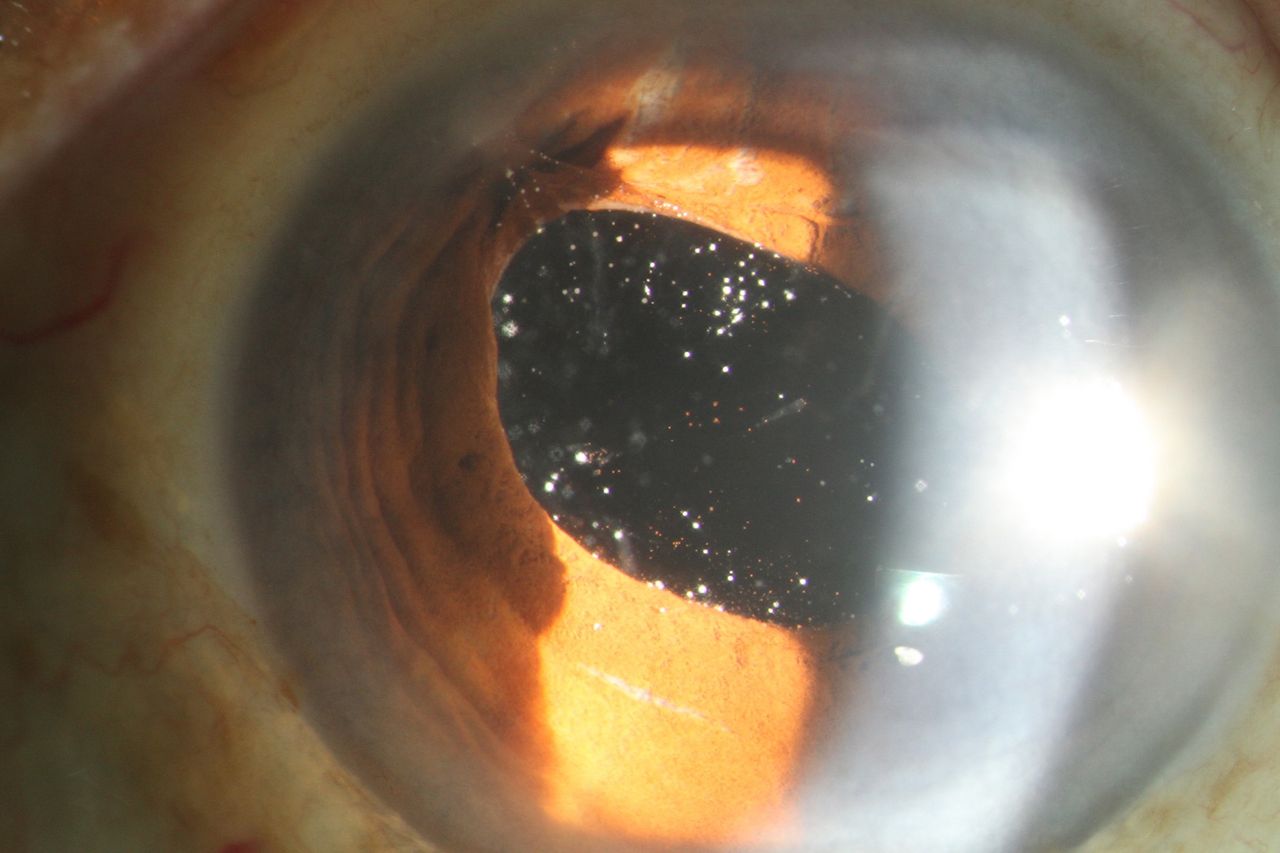
Anterior segment photo of the right eye shows prolapse of vitreous in the anterior chamber with incarceration in the inner lip of the superotemporal incisional scar, causing peaking of the pupil at 10 o’clock and temporal decentration of the intraocular lens. Multiple pigments and white dots appearing like asteroid hyalosis are seen in this vitreous framework.
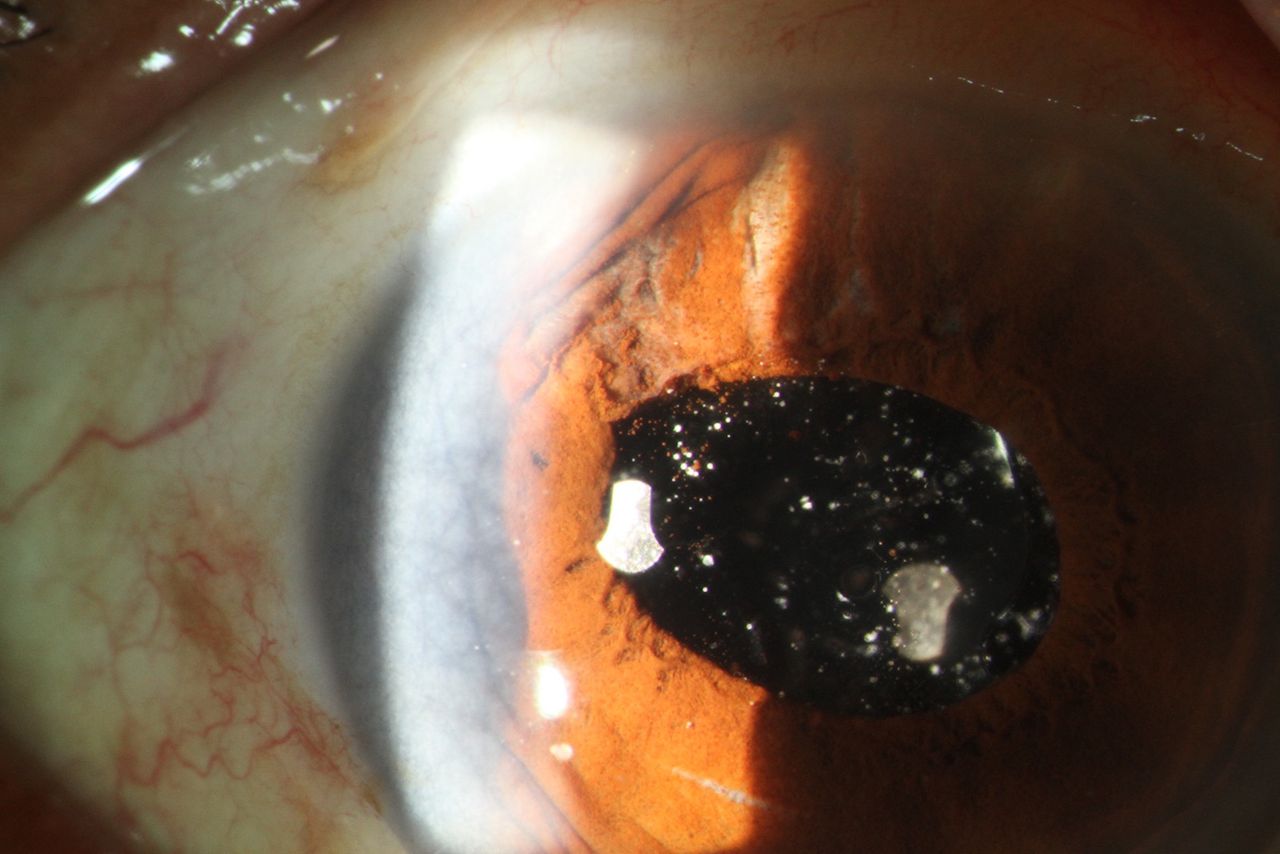
The anterior incarcerated vitreous was lysed using Nd:Yag laser. Following this the best-corrected vision improved to 20/40, N6 with vitreous and AH retracted to the iris plane (figure 2). Optical coherence tomography scan of the right eye macula did not show the presence of cystoid macular oedema. As clinically there was a clear view of the prolapsed AH in the anterior chamber via a posterior capsular defect, an ultrasound biomicroscopy pre-Nd:Yag and post-Nd:Yag laser was not performed.
{kind=link}
{kind=link}
Post-Nd:Yag vitreolysis, separation of the incarcerated vitreous from the surgical port is seen with retraction of vitreous and asteroid bodies to the iris plane.
AH is relatively uncommon degenerative ocular condition usually seen unilaterally in elderly individuals with a prevalence of up to 1.2%. They are seen as yellow-white bodies floating in the formed vitreous in chains or sheets, usually without visual compromise.1 Anomalous vitreoretinal adhesions are seen in eyes with AH where posterior vitreous detachment is uncommon and if occurs might lead to vitreoschisis or residual posterior vitreous cortex.2 Only two case reports of spontaneous prolapse of AH in the anterior chamber have been reported.3 4
Vitreous wicking syndrome is an uncommon condition where vitreous prolapses into the anterior chamber and passes through a wound breakdown with the formation of a wick onto the ocular surface. This condition is reported in cataract surgery with a posterior capsular defect, corneal relaxation incisions and intravitreal injections, and is known to cause cystoid macular oedema, vitreomacular traction, retinal detachment and endophthalmitis.5–8 This condition and prevention of associated complications can be treated medically, surgically or using ND:Yag vitreolysis.9 10
We report a case of vitreous with AH incarceration in the limbal surgical port following an eventful cataract surgery possibly causing an increased risk of vitreoretinal interface disorders as described above. This was successfully managed by using Nd:Yag vitreolysis to relieve the additional traction caused by the incarcerated vitreous in eyes with AH. The possible reason for the reduced vision could be the anterior concentration of asteroid bodies closer to the nodal point of the eye in view of the anterior vitreous prolapse.11
Learning points
Along with vitreous, asteroid hyalosis (AH) can also enter the anterior chamber and into the surgical wound after an eventful cataract surgery.
There is an increased risk of vitreoretinal interface disorders in cases of AH with vitreous wicking.
Vitreous wicking can be successfully managed with Nd:Yag vitreolysis.
Footnotes
Contributors SD was involved in patient care, literature search, data acquisition, manuscript preparation and manuscript editing. AP was involved in manuscript preparation and manuscript editing. SS was involved in patient care and data acquisition. MS was involved in data acquisition and manuscript editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.