Article Text

Summary
Skull base osteomyelitis in the setting of granulomatosis with polyangiitis (GPA) is rare and entails significant diagnostic challenges. We present a case of a 65-year-old Caucasian man with a history of rheumatoid arthritis, off immunosuppression for 18 months, who presented with 2 years of chronic headaches, severe fatigue, saddle nose deformity and 20-kilogram unintentional weight loss. Maxillofacial CT revealed an extensive destructive sinonasal and erosive skull base process. Laboratory evaluation showed equivocal elevation of antiproteinase 3 antibodies with negative antineutrophil cytoplasmic antibody panel. Biopsy of the skull base/clivus revealed necrotising granulomatous inflammation with focal vasculitis consistent with GPA, and multiple bone cultures were positive for Pseudomonas aeruginosa. This patient was diagnosed concurrently with GPA and P. aeruginosa skull base osteomyelitis. He was started on a 6-week course of cefepime intravenously and oral prednisone, with the plan to initiate rituximab infusion 2 weeks after initiation of antibiotic therapy.
- bone and joint infections
- vasculitis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Skull base osteomyelitis is defined as an inflammatory condition of the bone that begins with infection of the medullary bone, which then spreads to involve the haversian systems and periosteum. It is rare, but life-threatening, and it typically occurs in the setting of malignant otitis externa in patients with diabetes.1 2 Atypical presentations can present with primary headache without otic symptoms if patients have predisposing chronic sinonasal inflammation.1
Granulomatosis with polyangiitis (GPA) is an idiopathic small to medium vessel vasculitis.3 GPA classically presents with a triad of nasopharyngeal, pulmonary and renal symptoms.3 Otorhinolaryngological manifestations are the first symptoms of GPA in over 80% of patients.3 Although GPA is difficult to diagnose, up to 90% of correctly identified patients experience improvement in symptoms when treated appropriately with immunosuppressive medications.4 When disease is limited to the ear, nose and throat region, positive levels of antineutrophil cytoplasmic antibody (c-ANCA) may be present in only 46%–70% of patients.3 5
Early diagnosis and treatment of both GPA and skull base osteomyelitis is crucial to prevent morbidity and mortality.6 This case report highlights the diagnostic difficulties faced when considering nasopharyngeal GPA and skull base osteomyelitis. Furthermore, it raises the awareness for clinicians to have a low threshold suspecting these diagnoses if the clinical picture fits. Finally, we emphasise the need to exclude skull base osteomyelitis before starting immunosuppressive therapy for nasopharyngeal GPA.
Case presentation
A 65-year-old Caucasian man with a background of rheumatoid arthritis previously on adalimumab, with the last use 18 months prior to presentation, was admitted for management and work-up of chronic, recurrent nasopharyngeal destruction of unclear aetiology. The patient had a long history of sinus and occipital headaches for 2 years prior to presenting at our institution. He reported several episodes of severe epistaxis 1 year ago and underwent nasopharyngeal debridement that revealed abscess and osteomyelitis with erosions at the clivus. Prior cultures and histopathology of the abscess at an outside medical facility were negative for microbial growth and malignancies, respectively. Saddle nose deformity was noticed at this time. Reportedly, GPA was suspected, but the ANCA panel was negative and the diagnosis of GPA was not made. At the outside medical facility, the patient had been empirically treated with intravenous penicillin for 2 months, then intravenous ampicillin for 4 months for presumptive osteomyelitis. The patient had also been initiated on empiric voriconazole due to necrotic findings on histopathology, despite no evidence of fungal infection on histopathology stains or fungal cultures.
MRI of the head and neck showed sinus disease with invasion of skull base and no improvement after antimicrobial therapy. Voriconazole was subsequently changed to isavuconazole; in addition, he was initiated on doxycycline and levofloxacin. Despite these measures, the patient continued to deteriorate clinically. He became bedridden due to fatigue, and had developed hearing loss and oral ulcers. It was at this point that the patient presented to our institution, was found to be hypotensive in the outpatient setting and was admitted for further work-up.
On admission, the patient was cachectic, severely drowsy, but was arousable and answered questions. There was no rhinorrhoea and no signs of infection on nasal examination. He was hypotensive with a systolic and diastolic blood pressure of 70 mm Hg and 50 mm Hg, respectively. Physical examination including cardiopulmonary and neurological examination was otherwise unremarkable.
Investigations
On initial presentation, complete blood count was significant for haemoglobin of 10.6 (13.5–17.5 g/L), leucocytes of 9.3 (3.5–10.5×109/L), erythrocyte sedimentation rate of 71 (0–22 mm/hr), serum calcium of 10.7 (8.9–10.1 mg/dL), rheumatoid factor of 347 (<15 IU/mL), C reactive protein of 132(<8 mg/L) and anti- cyclic citrullinated peptide (anti- CCP) antibody of 221.2 U (<20 U). c-ANCA and p-ANCA tests were negative; however, proteinase 3 (PR3) ANCA was equivocal at 0.7 U (0.4–0.9 U considered equivocal). Serum creatinine on initial evaluation was 1.1 mg/dL (0.8–1.3 mg/dL). Estimated glomerular filtration rate by Cockcroft-Gault calculation was 47 mL/min. Urinalysis demonstrated no haemoglobinuria or proteinuria. Urine microscopy was normal and showed no evidence of haematuria.
CT of the skull base revealed extensive destructive sinonasal and skull base process with chronic osseous inflammatory changes and areas of osseous sinonasal and skull base dehiscence and erosion. Mucosal thickening was evident in the residual paranasal sinuses. These findings were suggestive of severe inflammatory disease such as GPA and/or chronic osteomyelitis.
MRI of the skull base revealed findings compatible with osteomyelitis of the skull base, right greater than left involvement, illustrated in axial T1 weighted images (T1WI) in figure 1A.
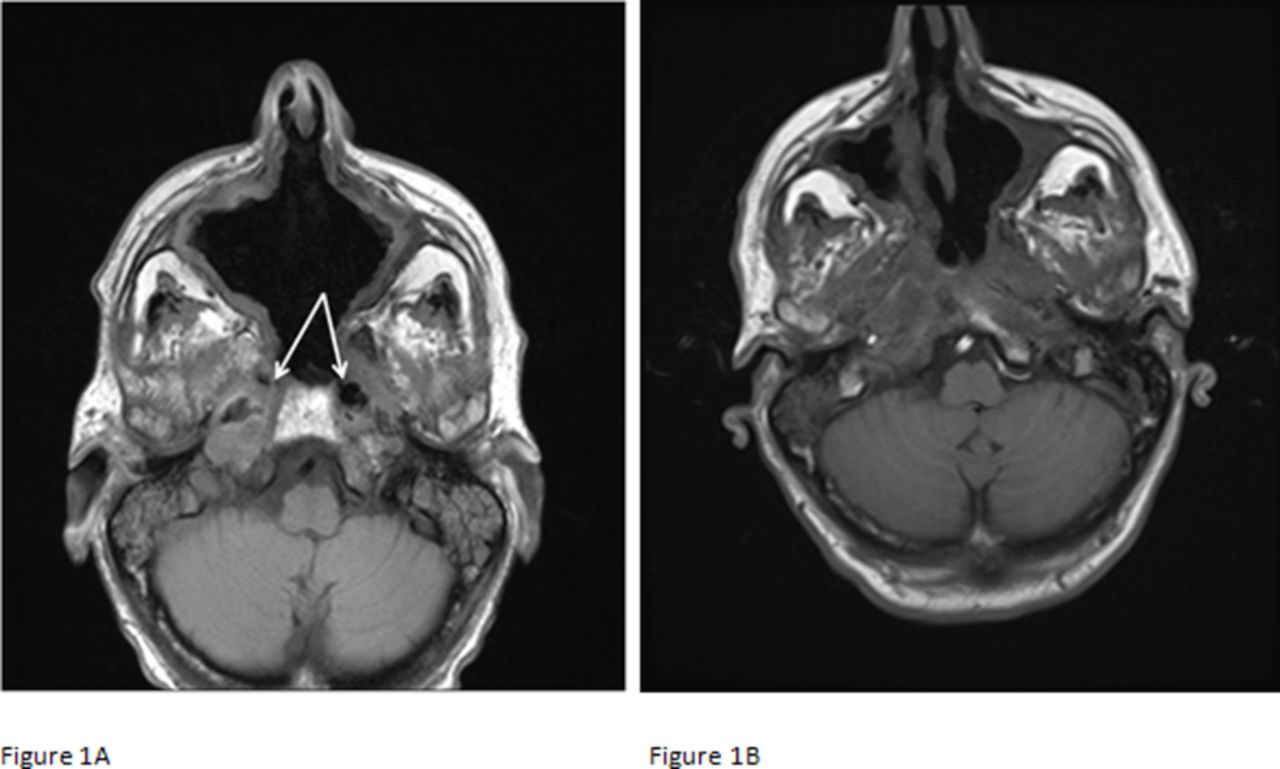
(A) Axial T1 weighted image (T1WI) demonstrates loss of normal marrow signal at the skull base on either side of the clivus. There are gas and debris in the soft tissues extending from the nasopharynx to the skull base indicating necrosis. Note the abnormal common cavity between the sinus and nasopharynx from the destructive process. (B) Axial T1WI demonstrating infiltrating abnormal signal obliterating the normal fat planes at the medial aspect of the masticator space, involving the soft tissues of the nasopharynx and loss of the normal marrow signal at the skull base, all compatible with infectious involvement. Destruction of the nasal septum and right maxillary sinus wall, as well as the ethmoid air cell septae, is also partially visualised on this image.
Axial T1WI MRI (figure 1B) further shows loss of the normal marrow signal at the skull base and destruction of the nasal seputm, right maxillary and ethmoid sinuses.
Surgical biopsies of the nasal soft tissue, frontal bone and clival bone were sent for culture and histopathology. Intraoperative findings revealed extensive destruction of all bone and cartilage within the nasal cavity. There was exposure of tooth roots and carotid artery in the maxillary sinus and skull base, respectively.
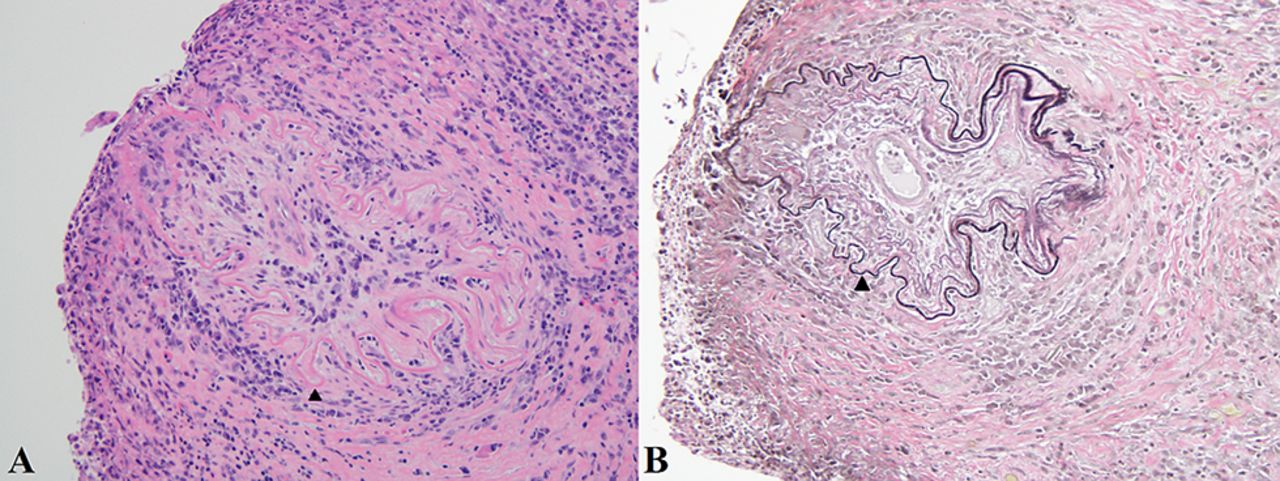
Biopsy of the nasal cavity, H&E slide shown in figure 2, reveals a poorly formed granuloma with palisading histiocytes shown at the arrowhead. Figure 3 reveals an area of leucocytic vasculitis demonstrated by (A) H&E stain and (B) Verhoeff-Van Gieson stain, highlighting infiltration of the elastic lamella of the vessel at the arrowhead. Multiple cultures of the biopsy revealed growth of fluoroquinolone-resistant Pseudomonas aeruginosa. Acid-fast bacilli and Grocott-Gomori’s methenamine silver stains were negative for mycobacterial and fungal organisms, respectively.

Microscopic examination of nasal cavity tissue shows a poorly formed granuloma with palisading histiocytes (arrowhead).

{kind=link}
{kind=link}
{kind=link}
An area of leucocytic vasculitis shown by (A) H&E stain and (B) Verhoeff-Van Gieson (VVG) stain. Infiltration through the vessel’s elastic lamella (arrowhead) is highlighted in the VVG stain.
Differential diagnosis
Malignancy
Osteomyelitis
GPA
Other vasculitides
Treatment
The patient’s hypotension responded to intravenous fluids. After the patient became clinically stable, he received debridement and irrigation of the nasal cavity, with subsequent initiation of a 6-week course of intravenous cefepime. The patient was also started on a course of prednisone. Rituximab infusion was arranged to be initiated 2 weeks after antibiotic therapy had been completed.
Outcome and follow-up
Follow-up with an MRI of the head and neck was arranged for 6 weeks following discharge.
Discussion
GPA is an idiopathic small to medium vessel vasculitis.3 It was previously termed Wegener’s granulomatosis, who described the triad of findings in 1936 including necrotising granulomatous inflammation and vasculitis of the upper respiratory tract and lungs, disseminated vasculitis affecting primarily small arteries, and glomerulonephritis.4 Patients typically present with symptoms involving the nasopharynx and lungs.4 Nasopharyngeal symptoms can range from uncomplicated sinusitis to epistaxis and destruction of the bony walls of the sinuses.4 Pulmonary symptoms may consist of chest pain, cough and haemoptysis.4 Patients can also present with otic involvement, which can cause sensorineural deafness.4 The glomerulonephritis usually manifests as haematuria and is typically a late manifestation of the disease.4 Some cases of GPA are limited to one area, and if symptoms are limited to otorhinolaryngological symptoms, the term ‘limited GPA’ is used.3
GPA is a difficult entity to diagnose, highlighted by a report that the time to diagnosis has not decreased in the UK from 2004 to 2014.7 The American College of Rheumatology has published diagnostic criteria for GPA. The four criteria include nasal or oral inflammation; chest imaging revealing nodules, fixed infiltrate or cavities; urinary sediment with haematuria or red cell casts; and granulomas within an artery or in the perivascular area of an artery or arteriole on biopsy.8 If two of the four criteria were met, the sensitivity for GPA was reported as 88% and the specificity as 92%.8 The definition of GPA adopted at the 2012 International Chapel Hill Consensus Conference on the Nomenclature of Vasculitides is ‘necrotizing granulomatous inflammation usually involving the upper and lower respiratory tract, and necrotizing vasculitis affecting predominantly small to medium vessels. Necrotizing glomerulonephritis is common’.9 The sinonasal mucosa is the site most often biopsied; this reveals the complete triad of vasculitis, necrosis and granuloma 15%–50% of the time in cases of GPA.4 Other associated diagnostic features include elevated inflammatory markers and ANCAs, particularly antibodies to PR3.3 4 However, absences of elevation of any of these markers do not exclude active disease, and as discussed above, when disease is limited to the ear, nose and throat region, positive c-ANCA levels may occur in only 46%–70% of patients.3 5 Contemporary practice to diagnose GPA usually relies on evidence of an ANCA and biopsy of affected organ.3
Treatment of GPA is divided into induction and maintenance phases.3 The mainstay of treatment had been cyclophosphamide and corticosteroids.4 Up to 90% of patients experience improvement in symptoms and 75% experience remission with this regimen.4 Rituximab therapy has recently been shown to be as effective as continuous conventional immunosuppression for induction and maintenance of remission over 18 months.10
Given the potential morbidity and mortality associated with destructive nasopharyngeal GPA, clinicians should have a high index of suspicion to facilitate timely diagnosis and treatment.3 6 GPA can mimic the MRI findings of skull base osteomyelitis.1 Fluorodeoxyglucose (FDG)-positron emission tomography (PET) scans have recently been investigated for the diagnosis of vasculitis in patients with active disease and can be useful, particularly when biochemical findings are equivocal.11 This imaging modality was not used in this case, but may have provided a diagnostic clue.
Skull base osteomyelitis is a life-threatening entity that results from chronic, inadequately treated infection.1 2 The typical pathophysiology of skull base osteomyelitis is contiguous spread of P. aeruginosa secondary to malignant otitis externa in an older patient with diabetes.1 6 However, skull base osteomyelitis can occur without otic involvement and present with headache as the primary symptom.1 2 These atypical cases usually present with an underlying condition, such as a chronic inflammatory sinonasal disease, and they presumably arise secondary to haematogenous spread or direct sinonasal seeding to destructed osseous tissue.1
The diagnosis of skull base osteomyelitis is made with presenting symptoms of persistent sinus discharge and tenderness, and confirmed by the presence of sequestrum or bony destruction on imaging.2 12 Biopsy with histopathology and culture provides the definitive diagnosis.2 Findings that should raise suspicion for skull base osteomyelitis include headache, cranial neuropathy, elevated erythrocyte sediment rate and abnormal clival imaging findings.1
The primary treatment of osteomyelitis is surgical debridement and irrigation.12 Long-term antibiotic therapy is the traditional adjunctive treatment, and the standard recommendation for treating chronic osteomyelitis is 6 weeks of parenteral antibiotics.12 13 However, the optimal duration of therapy remains uncertain.13 For chronic skull base osteomyelitis, some published literature suggests to continue antibiotics for up to 6 months, much longer than usual for odontogenic infections.2
There is a paucity of case reports of associations between vasculitides and osteomyelitis. Table 1 highlights the published case reports within the past 20 years. A literature review was completed with Medical Subject Headings (MeSH) search terms of ‘vasculitis’ and ‘osteomyelitis’ using PubMed search engine.
Case reports of vasculitis associated with osteomyelitis
A recent case report by Harrison et al14 highlighted in the above table, identifies the importance of recognising that nasopharyngeal GPA can mimic skull base osteomyelitis. Our case is an important complementary follow-up to ensure clinicians are aware of the potential of a superimposed infectious pathology, and the need to exclude osteomyelitis before empirically treating a vasculitis with immunosuppression prior to completion of an appropriate antibiotic course. Immunosuppression has been identified as a risk factor for early death in skull base osteomyelitis.15
To our knowledge, this is the first case report of skull base osteomyelitis superimposed on chronic nasopharyngeal GPA. This case highlights the importance of investigating GPA or other associated vasculitides in the setting of skull base osteomyelitis as it will change the therapeutic approach and outcomes in our patients.
Learning points
Clinicians should have a high suspicion of granulomatosis with polyangiitis (GPA) or other associated vasculitides with chronic destructive sinus disease, even with normal or equivocal antineutrophil cytoplasmic antibodies.
Destructive nasopharyngeal GPA can lead to superinfection with osteomyelitis.
Prompt diagnosis is crucial to prevent severe morbidity in destructive nasopharyngeal GPA and skull base osteomyelitis.
It is essential to exclude underlying infection before initiating empiric immunosuppression for GPA.
References
Footnotes
Contributors MSvI, JPA, DDS and JAW contributed to the conception and design of this case report, interpretation of data, critical revision and final approval of the manuscript. All authors agree to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved.
Competing interests None declared.
Patient consent Obtained from guardian.
Provenance and peer review Not commissioned; externally peer reviewed.