Article Text

Statistics from Altmetric.com
Description
A 36-year-old man with no medical history, consulted for a 2-week onset right-sided retro-orbital pain associated with diplopia. On neurological examination the patient had combined ipsilateral third and fourth cranial nerve palsy and hypoesthaesia in the distribution of V1 of the trigeminal nerve.
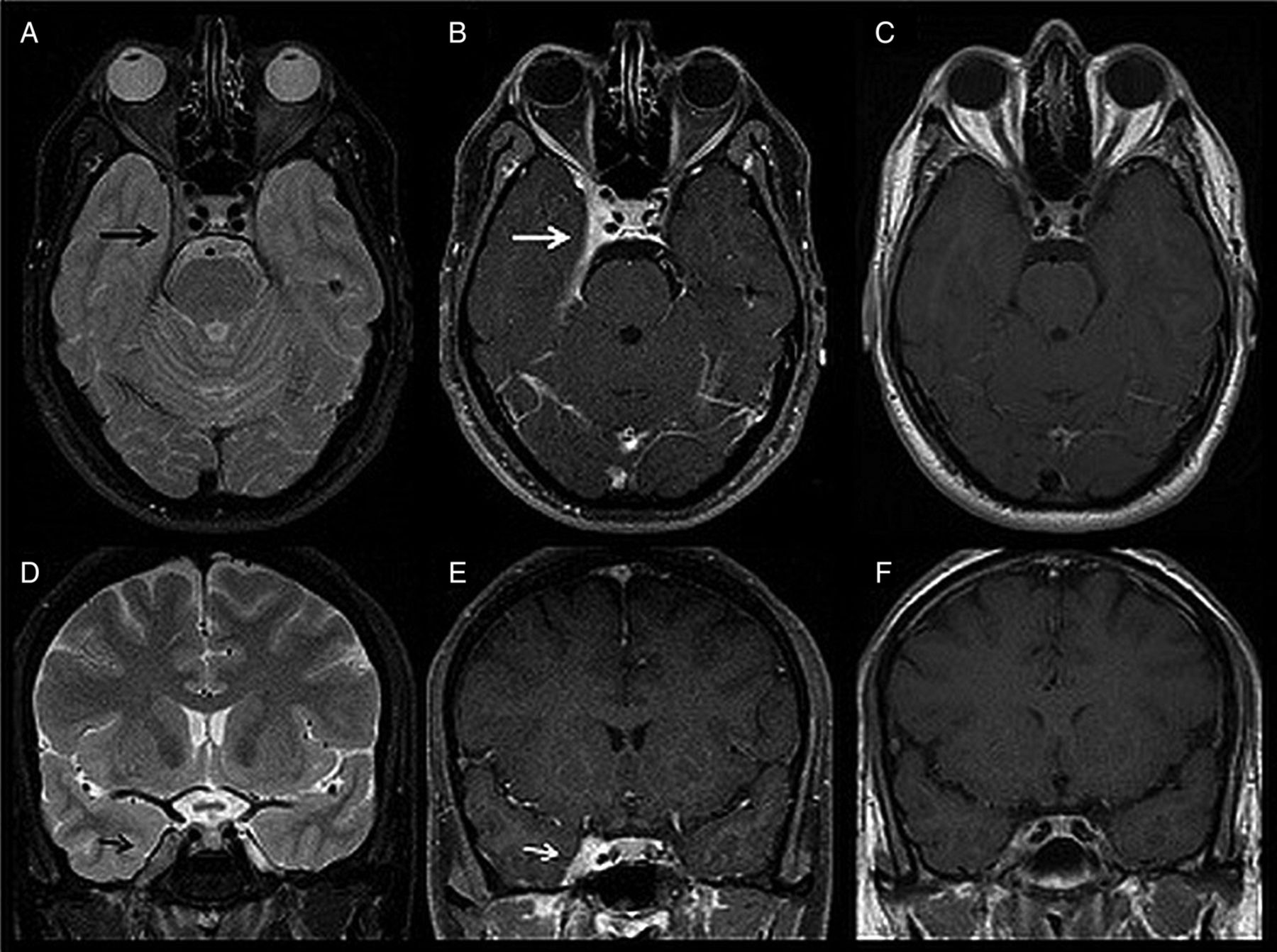
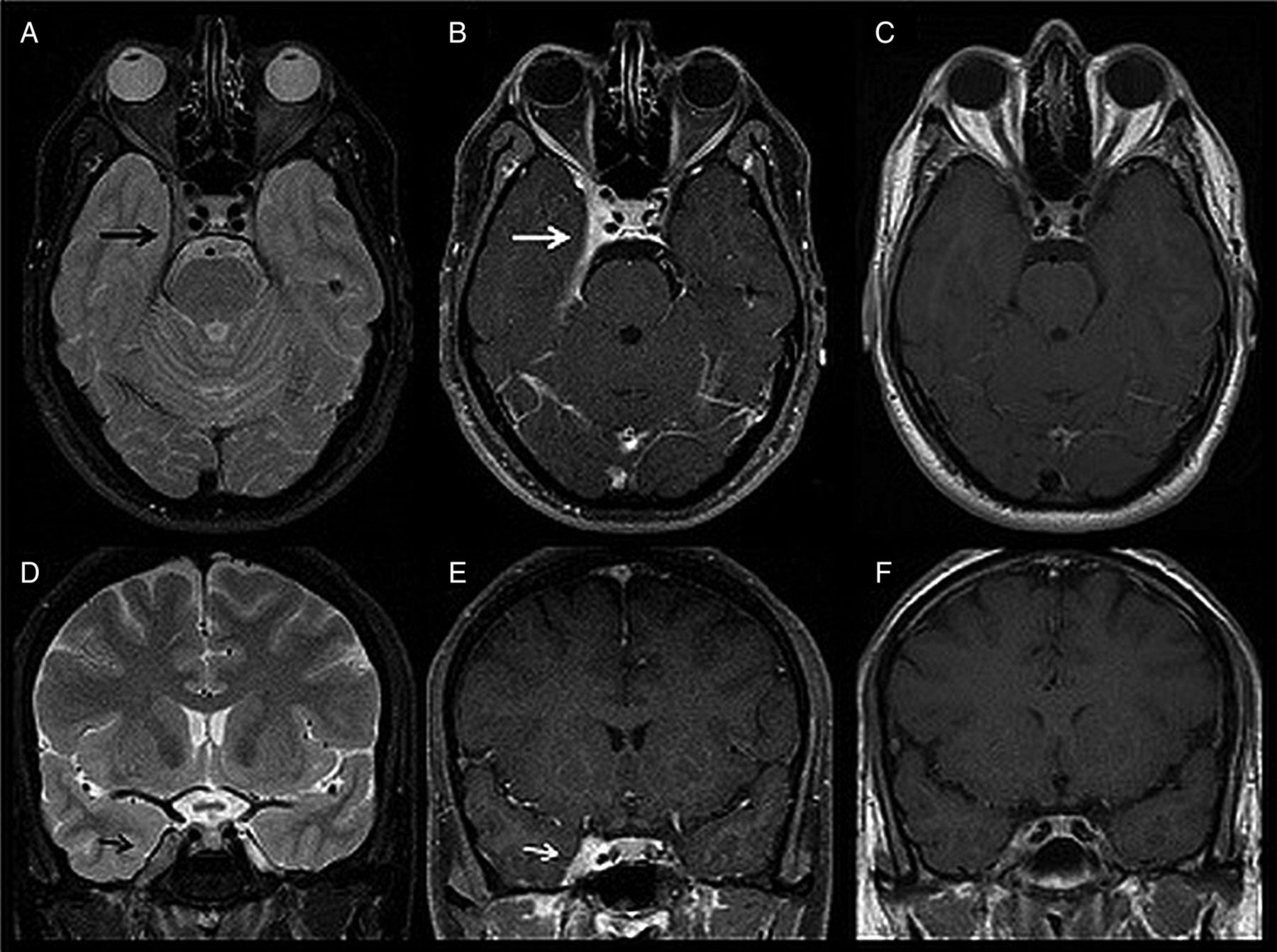
Brain MRI demonstrated abnormal enlargement and enhancement of the right cavernous sinus (CS) extending through the superior orbital fissure into the orbital apex (figure 1). Other infectious, inflammatory, neoplastic and vascular entities involving the CS were excluded by appropriate investigations. The painful ophthalmoplaegia had a prompt response to steroid therapy (within 72 h) and follow-up brain MRI demonstrated significant improvement (figure 1).
{kind=link}
MRI finding of a 36-year-old male patient with right-sided Tolosa-Hunt syndrome. Axial (A) and coronal (D) T2-weighted images (WI) show an enlarged right cavernous sinus (CS) that is mildly hypointense to grey matter (black arrow). Axial (B) and coronal (E) postcontrast T1-weighted fat-suppressed images show the enhancement of the abnormal soft tissue extending through the superior orbital fissure into the orbital apex (white arrow). Also noted is the hyperenhanced thickening of the right temporal dura, tentorium and right orbital apex. Axial (C) and coronal (F) postcontrast T1-WI follow-up, performed one month later, show significant improvement of right-sided CS abnormal enlargement and enhancement.
Tolosa-Hunt syndrome (THS)1 is an idiopathic inflammatory granulomatous process involving the CS with possible extension into the superior orbital fissure and orbital apex. The inflammation causes extrinsic compression of the neurovascular structures that cross the CS. THS clinical presentation consists of relapsing unilateral painful ophthalmoplegia, which is responsive to steroid therapy.2
Gadolinium-enhanced MRI is the imaging modality of choice to evaluate THS and may demonstrate abnormal enlargement and enhancement of the CS extending through the superior orbital fissure into the orbital apex. Reported MRI findings on T1-weighted and T2-weighted images are extremely variable and non-specific.3
MRI plays a pivotal role in diagnosing and helps to exclude other common lesions involving the CS, avoiding the need for high-risk invasive procedures such as a biopsy of the SC, the only way to obtain the histopathological confirmation of this disease.
Learning points
-
Tolosa-Hunt syndrome (THS) diagnosis is based on clinical manifestations, rapid response to steroids, MRI findings and exclusion of other causes of cavernous sinus (CS) involvement.
-
Gadolinium-enhanced MRI is the imaging modality of choice to evaluate the THS and may demonstrate abnormal enlargement and enhancement of the CS extending through the superior orbital fissure into the orbital apex.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.