Article Text

Summary
Highly active antiretroviral therapy (HAART) has dramatically improved the morbidity and mortality of patients with HIV. Although the incidence of AIDS-defining neoplasms is decreasing with this therapy, they must still be considered in patients who present with suspicious symptoms. Early diagnosis and treatment may help to improve quality of life and clinical outcome. We report the case of a 30-year-old man on HAART who presented with an expanding lump in the left groin, thought to be a haematoma for 5 months. A high level of suspicion led to a prompt diagnosis of Burkitt's lymphoma followed by timely treatment with chemotherapy. This culminated in complete remission, with an improved quality of life.
Statistics from Altmetric.com
Background
A lump in the groin can be a common clinical presentation for an active, healthy person. The differential diagnoses include an inguinal or femoral hernia, inguinal lymphadenopathy, a saphena varix and, rarely, a haematoma. Prior to highly active antiretroviral therapy (HAART), a patient with HIV presenting with a painless lump in the groin, neck or axilla would be strongly suspected of having an AIDS-defining illness, and the appropriate management would be commenced without delay. HAART has revolutionised the treatment of HIV in many ways. Typically consisting of two nucleoside reverse transcriptase inhibitors and either a non-nucleoside reverse transcriptase inhibitor (NNRTI), protease inhibitor or integrase inhibitor, combination therapy helps to minimise drug resistance, reduce viral burden and preserve immune system function. As a result, mortality from AIDS-defining illnesses, including opportunistic infections and AIDS-related malignancies, has decreased, with a corresponding increase in mortality from non-AIDS-defining illnesses such as colorectal and anal cancers, and hepatic, cardiovascular and pulmonary disease.1 ,2 In light of these advances, it is possible that the clinical suspicion for an AIDS-defining illness is not as high in the present day as it was prior to the era of antiretrovirals and HAART. This case report demonstrates that the suspicion for an AIDS-defining illness must remain high in patients who clinically and objectively demonstrate a good response to HAART. Moreover, it encourages clinicians to consider an AIDS-defining illness as the primary diagnosis in individuals on HAART who present with innocuous symptoms. This will minimise diagnostic delay and permit treatment to be initiated quickly.
Case presentation
A 30-year-old man attended the emergency department with a slowly expanding mass in the left groin. Five months prior to his presentation he had sought advice from his primary care physicians, who felt it was a haematoma caused by a minor injury sustained at the gym. When the mass did not resolve, another general practitioner referred him to the general surgical emergency service for evacuation of the suspected haematoma. The man was a fit, athletic individual with HIV who was otherwise well, with no constitutional symptoms such as weight loss, fevers or night sweats. He had been taking HAART for 9 months following a CD4 count that had fallen to 340 cells/mm3. On admission, his CD4 count was 560 cells/mm3 and his viral load was undetectable, indicating that HAART was producing a good biological response.
On clinical examination, the mass measured 15×10 cm. It was tender and firm with induration of the overlying skin. The left leg and thigh was enlarged with non-pitting oedema and suggested lymphoedema. Chest and abdominal examination, including digital rectal examination, was unremarkable.
Investigations
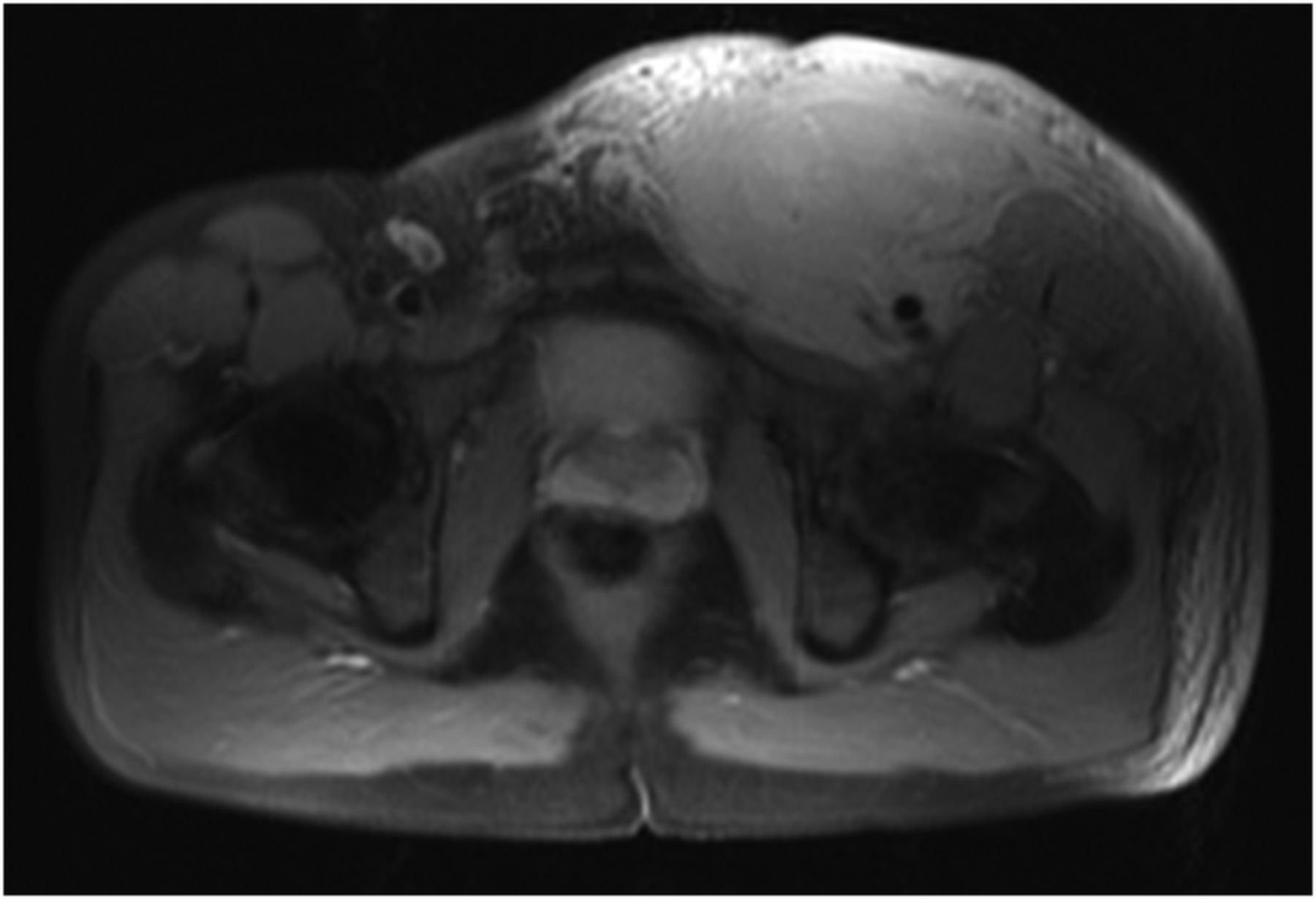
On admission, the serum lactate dehydrogenase (LDH) was elevated; all other routine blood haematological and biochemical analysis was unremarkable (Table 1). A CT scan revealed an isolated, irregular mass in the left groin, measuring 14×11 cm, with associated fat stranding and invasion of the adjacent musculature (figure 1). The mass also encased the femoral vessels and a Doppler ultrasound confirmed thrombosis of the common femoral and long saphenous veins. The CT scan of the chest, abdomen and pelvis was otherwise unremarkable. MRI showed the mass to be multi-septate, containing patchy areas of enhancement with an avid rim (figure 2).
Blood test results on admission, with laboratory reference ranges indicated in brackets

Transverse CT image demonstrating a large, irregular mass in the groin with encasement of the femoral vessels.

T2-weighted MRI image showing patchy uptake of gadolinium and an avid rim.
Histological analysis of multiple core biopsies revealed discohesive malignant cells with hyperchromatic moderately pleomorphic nuclei, granular chromatin and scanty cytoplasm, diffusely infiltrating a fibrofatty stroma. There were multiple areas of high mitosis and necrosis. On immunohistochemical staining, the biopsies were strongly positive for CD20, suggesting, together with the morphological appearances, high grade B cell lymphoma. In addition, the cells were strongly positive for CD10 and Bcl-6 but negative for Bcl-2 and MUM1. An MIB1 proliferation fraction approached 100%. In situ hybridisation demonstrated no evidence of Epstein-Barr virus (EBV)-encoded RNAs or a TP53 deletion. Similarly, there were no apparent rearrangements of BCL6, IGH/MYC or IGH/BCL2. The detailed histological assessment favoured a diagnosis of Burkitt's lymphoma.
A positron emission tomogram indicated the groin mass to be intensely fluorodeoxyglucose (FDG)-avid, with diffuse subcutaneous extension in the left thigh (figure 3). FDG-avid lymph nodes were present adjacent to the mass, in the left external iliac chain and bilaterally in the axillary and deep upper cervical regions (not detectable clinically).

{kind=link}
{kind=link}
{kind=link}
Positron emission tomogram demonstrating fluorodeoxyglucose uptake.
Treatment
The time from admission to formal diagnosis was 12 days. The patient was referred to the appropriate specialist team and commenced on chemotherapy.
Outcome and follow-up
The patient had a complete metabolic response to the chemotherapy. At 8 months follow-up, he remains in clinical and radiological remission and continues with his usual activities of daily living.
Discussion
This case report reiterates the importance of suspecting an AIDS-defining illness in patients on HAART who are otherwise clinically well, with preserved CD4 counts and undetectable viral loads. Maintaining a high index of suspicion for such conditions facilitates prompt diagnosis and treatment, potentially improving clinical outcome.
Lymphoma is one condition that defines a patient with HIV as having AIDS.3 Lymphomas frequently (>95%) arise from B cells and are categorised as shown in box 1.4 A key difference between lymphomas associated with HIV and those in the general population is that they are often more aggressive, with frequent spread to the bone marrow and extra-nodal tissues and organs. HAART, and the immune reconstitution that it provides, permits aggressive treatment of HIV-associated non-Hodgkin's lymphomas (NHLs); hence the reason why our patient was treated with chemotherapy in conjunction with ongoing HAART. Chemotherapeutic combinations that have been employed include CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone), dose-adjusted EPOCH (etoposide, prednisone, vincristine, cyclophosphamide and doxorubicin) and CODOX-M/IVAC (cyclophosphamide, vincristine, doxorubicin, methotrexate/ifosfamide, etoposide, cytarabine), all with or without rituximab.
Categories of AIDS-related lymphomas
A. Lymphomas that occur specifically in HIV-positive patients (eg, primary effusion lymphoma, plasmablastic lymphoma of the oral cavity type)
B. Lymphomas that also arise in immunocompetent patients (eg, Burkitt's lymphoma, diffuse large B cell lymphoma, classical Hodgkin's lymphoma)
C. Lymphomas that are also seen in other (non-HIV) immunocompromised states (eg, polymorphic B cell lymphoma (PTLD-like))
Adapted from Raphael et al.4
Multiple risk factors for developing an HIV-associated systemic NHL are described in the literature. A patient at low risk would be aged ≤35 years, on HAART, with high current and nadir CD4 counts, an undetectable viral load and no previous episodes of immunosuppression.5 The CD4 count has been shown in several studies to be the strongest indicator of lymphoma risk.5 ,6 In one study, patients with a CD4 count of <50 cells/mm3 had a 17-fold greater incidence of HIV-associated systemic NHL than patients with a CD4 count of ≥500 cells/mm3.5 Our patient had a CD4 count of 560 cells/mm3 at presentation. It is possible that lymphoma was considered to be low on the list of differential diagnoses as the patient's CD4 count, general welfare and ongoing treatment with HAART indicated a low risk of lymphoma. Importantly however, nearly a quarter of cases of HIV-associated NHL are diagnosed in patients with a CD4 count of ≥350 cells/mm3 and a tenth of cases are diagnosed in patients with a CD4 count of ≥500 cells/mm3.5 These levels of CD4 count should not therefore preclude a diagnosis of an AIDS-defining malignancy in patients with suspicious or unexplained symptoms and/or signs. Moreover, an HIV-positive patient on HAART remains at a much greater risk of developing lymphoma than the general population, with nearly five times as many HIV-positive patients dying from non-Hodgkin's lymphoma relative to controls in one prospective study.7 An elevated serum LDH (as was true of our patient) should heighten the awareness for lymphoma and ensure rapid referral to the appropriate speciality.8
Several factors are thought to contribute to the increased risk of lymphoma in HIV-positive patients. These include the propensity for cells to be transformed by HIV itself and opportunistic infection with viruses such as EBV.9 ,10 Although absent in the patient described here, EBV is present in 40–50% of HIV-associated lymphomas.4 ,9 In the case of Burkitt's lymphoma, EBV is believed to encourage transformation through the promotion of genetic instability and protection of tumour cells against programmed cell death.10 It is possible that targeting EBV may provide another means of treating lymphomas associated with this virus. Novel approaches include targeting EBV-associated oncoproteins such as latent membrane protein-1 (LMP-1). Complete responses have been described in patients with EBV-associated lymphomas who received infusions of autologous cytotoxic T lymphocytes directed against the LMP-1 and LMP-2 antigens.11 Simvastatin, a medication frequently used in the treatment of hypercholesterolaemia, may also be of value. Simvastatin blocks key cell–cell interactions and induces apoptosis in EBV-transformed B lymphocytes and has been shown to delay the development of EBV-associated lymphomas in immunocompromised mice.12 ,13
Strategies to further reduce the incidence of HIV-associated NHLs must take into account the significant proportion of cases that arise in patients with CD4 counts of ≥350 cells/mm3.5 Whereas current British HIV Association guidelines recommend initiation of HAART in patients with CD4 counts of ≤350 cells/mm3,14 recent International Antiviral Society-USA guidelines suggest offering HAART to all HIV-positive patients, irrespective of CD4 count.15 Given that 25% of new cases of HIV are diagnosed in individuals with CD4 counts of ≤200 cells/mm3, there must also be a drive to promote early diagnosis of HIV infection.5 ,6 ,16 The UK National Guidelines for HIV Testing now recommend considering HIV testing in all people attending sexual health clinics, antenatal services and drug dependency programmes, as well as patients registering with general practices and attending hospitals in areas of high HIV prevalence (exceeding 2 in 1000 population).16
An important consideration in the treatment of patients with HIV-associated malignancies is the potential for drug interactions when using antineoplastic agents and HAART concomitantly. Protease inhibitors are known to delay clearance of antineoplastic agents, including cyclophosphamide, through inhibition of cytochrome P450-mediated metabolic pathways.17 ,18 Furthermore, NNRTIs are metabolised via the cytochrome P450 system and, as such, may interact with antineoplastic agents utilising the same metabolic pathways, for example vincristine.18 Careful drug selection and close monitoring are essential if toxic accumulation (or unwanted, enhanced clearance) of antineoplastic agents is to be avoided. In this regard, an important development has been the introduction of integrase inhibitors, such as raltegravir, into HAART regimens for patients receiving treatment for HIV-associated lymphomas. In one study, use of raltegravir in patients with HIV-associated malignancies was associated with fewer adverse effects when compared to protease inhibitors and NNRTIs.19 Efficacy, in terms of maintaining viral suppression at 6 months, was comparable between raltegravir and NNRTIs and superior to protease inhibitors. The authors of the study suggested that integrase inhibitors should be considered as first-line antiretroviral agents for HIV-positive patients with haematological malignancies or those patients receiving antineoplastic agents.
The case report presented highlights the potential problem faced by primary care and hospital physicians not regularly exposed to HIV and its associated conditions. A slow-growing, painless, solitary groin lump with no other lymphadenopathy on clinical examination could easily be mistaken for a benign lesion in a patient on HAART with acceptable CD4 counts. There should be a low threshold for referral to the appropriate speciality in such patients. Adopting this policy would minimise delay in diagnosis, permit early treatment and potentially improve outcome.
Learning points
-
Relative to the general population, patients with HIV on highly active antiretroviral therapy (HAART) remain at a greatly increased risk of developing AIDS-defining malignancies.
-
Therefore, clinicians should maintain a high index of suspicion for AIDS-defining malignancies in patients on HAART with acceptable CD4 counts and undetectable viral loads.
-
Approximately one quarter of cases of HIV-associated systemic non-Hodgkin's lymphomas are diagnosed in patients with a latest CD4 count of ≥350 cells/mm3.
-
An HIV-positive patient presenting with a mass in a lymphatic distribution should be viewed as having a lymphoma until proven otherwise, irrespective of CD4 count or viral load, and whether or not the patient is on HAART.
-
HIV-positive patients should be encouraged to be vigilant in reporting any new lumps or bumps to their physician as early diagnosis and rapid treatment may allow improved survival.
References
Footnotes
-
Contributors MDR, DS-R and JC all contributed to: conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.