Article Text

Statistics from Altmetric.com
Description
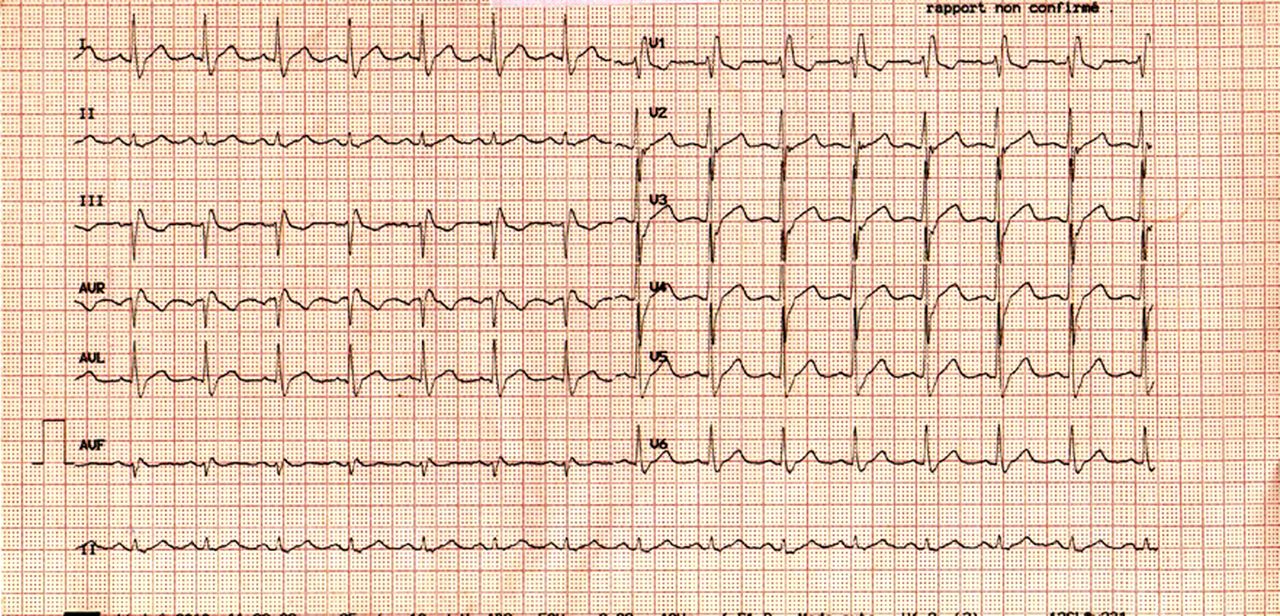
A 62-year-old patient was admitted to our department for fatigue and chest discomfort. He had a history of multiple myeloma and systemic hypertension. Blood pressure, heart rate and physical examination were unremarkable. ECG demonstrated a normal sinus rhythm with a right bundle branch block (figure 1). Blood was sampled and cardiac troponin (cTn) I was persistently increased from 2.8 to 3 ng/ml (Beckman Coulter Access II and DXi 800 platforms, Beckman Coulter Inc, Fullerton, California, USA). Left ventricular ejection fraction was normal at 0.60 with a trace of aortic regurgitation at transthoracic Doppler echocardiography. Coronary angiography revealed the absence of significant luminal narrowing on epicardial arteries (figure 2 A,B). A monoclonal peak of IgG was found at serum protein electrophoresis (figure 3). Rheumatoid factor was undetectable. Alanine aminotransferase and aspartate aminotransferase or amylase levels were within the normal range. No fibrin clot was present in the blood sample and the blood was not apparently viscous. The lipemic index was low at 1 (range from 1 to 15) and there was no haemolysis. Serum of the patient was hence mixed with an equal proportion of polyethylene glycol (PEG) 6000, 250 g/l. The solution was incubated at 37°C during 10 min, then centrifuged 10 min at 5000 rpm. cTnI activity was reassessed within the supernatant and remained undetectable.

Twelve lead surface ECG demonstrating a right bundle branch block.

Coronary angiography showing absence of coronary artery narrowing in left (A) and right (B) coronary arteries.

{kind=link}
{kind=link}
{kind=link}
Serum protein electrophoresis showing a monoclonal peak of IgG lambda at 11.9 g/dl.
An unexpected rise in cTnI may occur in various clinical settings other than coronary artery disease, such as pulmonary embolism, sepsis or stress-induced cardiomyopathy. In the present case, the unexpected rise in serum cTnI disappeared after PEG precipitation. Elevated cTnI concentration was attributed to cTnI being sequestered as a high molecular mass (macro) enzyme complex with serum IgG rather than a result of increased cTnI released by damaged myocardial tissue.1 Hence, clinicians should pay attention to immunocomplexes involving cTnI and proteins as IgG producing false-positive cTnI in patients with mutiple myeloma. We acknowledge that PEG precipitation has some pitfalls2 and does not specifically remove macro cTnI. In addition, PEG precipitation does not identify the mechanism of the interaction between the monoclonal peak and cTnI. In addition, we did not demonstrate in the present case cTnI removal by protein A, protein G or antihuman immunoglobulin,3 as the clinical course of the patient including normal coronary angiography, did not motivate us to perform additional analyses. Nevertheless, PEG precipitation of IgG followed by other confirmatory techniques may help unveil the absence of ‘true’ increased serum cTnI concentration and avoid invasive procedures that may be harmful in these frail patients.
Learning points
-
Increased serum cTnI concentration does not always reflect myocardial injury.
-
Elevated cTnI concentration may be related to cTnI being sequestered as a high molecular mass (macro) enzyme complex with serum IgG in patients with mutiple myeloma.
-
Polyethylene glycol precipitation of IgG followed by other confirmatory techniques may help unveil the absence of ‘true’ increased serum cTnI concentration in these patients.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.