Article Text

Summary
The present report describes the case of an 80-year-old woman who presented at the emergency department with progressive respiratory distress caused by a massive anterior neck mass with tracheal deviation and compression. A CT scan showed diffuse enlargement of the thyroid gland. The patient underwent a left-sided hemithyroidectomy. Pathology unexpectedly revealed a primary thyroid lymphoma. Treatment with prednisone and vincristine was initiated to reduce tumour size and preserve the airway, resulting in rapid volume reduction and airway expansion. Primary thyroid lymphoma is a rare entity that requires adequate diagnosis and rapid initiation of treatment to reduce tumour volume and to prevent airway compromise.
Statistics from Altmetric.com
BACKGROUND
This case report describes a patient who presented with progressive respiratory distress and inspiratory stridor based on a thyroid lymphoma. Primary lymphoma of the thyroid is an uncommon disease. The differential diagnosis of a rapidly expanding thyroid mass includes: goitre, abscess, infection, haemorrhage into a benign nodule, thyroiditis, anaplastic carcinoma, metastatic cancer, or thyroid lymphoma. Thyroid lymphoma can present with tracheal compressive symptoms due to an expanding thyroid mass, which can occur rapidly. This case highlights the urgency of early diagnosis and treatment of this aggressive thyroid malignancy. Early treatment also helps in limiting the effects of tracheomalacia. Although rare, a primary thyroid lymphoma has to be considered in the differential diagnosis of rapidly expanding thyroid mass with progressive respiratory distress. Rapid initiation of treatment can reduce tumour volume and prevent airway compromise. The prognosis usually is favourable because this condition typically presents with localised disease, which is amenable to treatment with chemotherapy and radiation.
CASE PRESENTATION
An 80-year-old woman presented to the emergency department having experienced progressive respiratory distress and inspiratory stridor for several months, which had worsened in the last 12 h. Her medical history revealed globus issues, dysphagia, symptoms of reflux oesophagitis and shortness of breath. She did not have thyroid disease. On arrival at the emergency room she developed respiratory arrest and collapsed and was successfully resuscitated with epinephrine 1 mg and atropine 0.4 mg and intubated. Initial assessment showed severe bradycardia (less then 20 beats per min) and immeasurable blood pressure. Arterial oxygen saturation (SaO2) was less than 80%.
Her initial arterial blood gas showed a severe metabolic and respiratory acidosis: pH 7.16 (normal range 7.35–7.45), partial CO2 p(CO2) 9.2 kPa (normal 4.5–6 kPa), HCO3 45 mmol/litre (normal 22–26 mmol/litre), pO2 15.7 kPa (normal 9.5–13 kPa), base excess (BE) –12.5 mmol/litre (normal –2 to 2 mmol/litre), O2 saturation 100%, lactate 9.2 mmol/litre (0.5–1.7 mmol/litre).
Intubation was difficult due to significant resistance after introduction of the endotracheal tube (ET) at 23–24 cm depth. She was admitted to the intensive care unit (ICU) for further management.
Vital signs were as follows: temperature 35.5°C, blood pressure 77/43 mm Hg, pulse 91 min−1, SaO2 95% on mechanical ventilation. Repeat blood gas analysis revealed pH 7.28, pCO2 6 kPa, PO2 11.5 kPa, HCO3 20.7 mmol/litre, BE −5.3 mmol/litre, sat 96%. Laboratory examinations showed: haemoglobin (Hb) 6.5 mmol/litre (normal 8.5–11 mmol/litre), haematocrit 0.31 litre/litre (normal 0.4–0.52 litre/litre), plately count 109 cells/nl (normal 150–400 cells/nl), white blood cell count 12.1×103 cells/g/litre (normal 4.3–10.8×103 cells/g/litre) Na 142 mmol/litre (normal 135–145 mmol/litre), K 3.9 mmol/litre (normal 3.5–4.7 mmol/litre), γ-glutamyl transferase 12 IU/litre (normal 0–50 IU/litre), alkaline phosphatase 53 IU/litre (normal 0–120 IU/litre), aspartate aminotransferase (ASAT) 54 IU/litre (normal 0–45 IU/litre), alanine aminotransferase (ALAT) 37 IU/litre (normal 0–45 IU/litre), Mg 1.18 mmol/litre (normal 0.70–1.10 mmol/litre), Ca2+ 1.12 mmol/litre (normal 1.15–1.29 mmol/litre), lactate dehydrogenase (LD) 519 IU/litre (normal 0–450 IU/litre), troponin I 0.40 μg/litre (normal <0.20 μg/litre), creatine kinase (CK) 54 IU/litre (normal 0–170 IU/litre), lactate 3.3 mmol/litre (normal 0.5–1.7 mmol/litre).
A control chest x ray post intubation showed good position of the endotracheal tube and tracheal deviation. There were no signs of pulmonary oedema or pulmonary infiltrates.
Physical examination revealed a palpable neck mass resembling diffuse goitre with a diameter of 7 cm. There were no palpable nodes. Thyroid function tests were normal, with free T4 15.2 pmol/litre (normal 10–24 pmol/litre) and thyroid stimulating hormone (TSH) 4.13 mU/litre (normal 0.4–4 mU/litre).
DIFFERENTIAL DIAGNOSIS
Pulmonary embolism was included in the differential diagnosis because of the progressive respiratory distress, the shortness of breath and the low oxygen saturation (80%), however the progressive and longstanding issues made this less likely. We also considered congestive heart failure as it often presents with respiratory distress and can ultimately lead to cardiac failure and collapse. However the negative chest x ray made the last diagnosis unlikely. The progressive globus issues and dysphagia, together with the difficult intubation, lead us to include laryngeal, hypopharyngeal or thyroid masses/malignancies in the differential diagnosis.
The differential diagnoses for neck mass are:
-
branchial cleft cyst
-
thyroglossal duct cyst
-
vascular tumour or malformation
-
laryngocele
-
ranula (mucocele or retention cyst)
-
teratoma
-
dermoid cyst
-
thymic cyst
-
lymphadenopathy (viral/bacterial)
-
neoplasm (thyroid, salivary gland)
-
paraganglioma (carotid body, glomus tumours)
-
schwannoma
-
lymphoma
-
lipoma.
INVESTIGATIONS
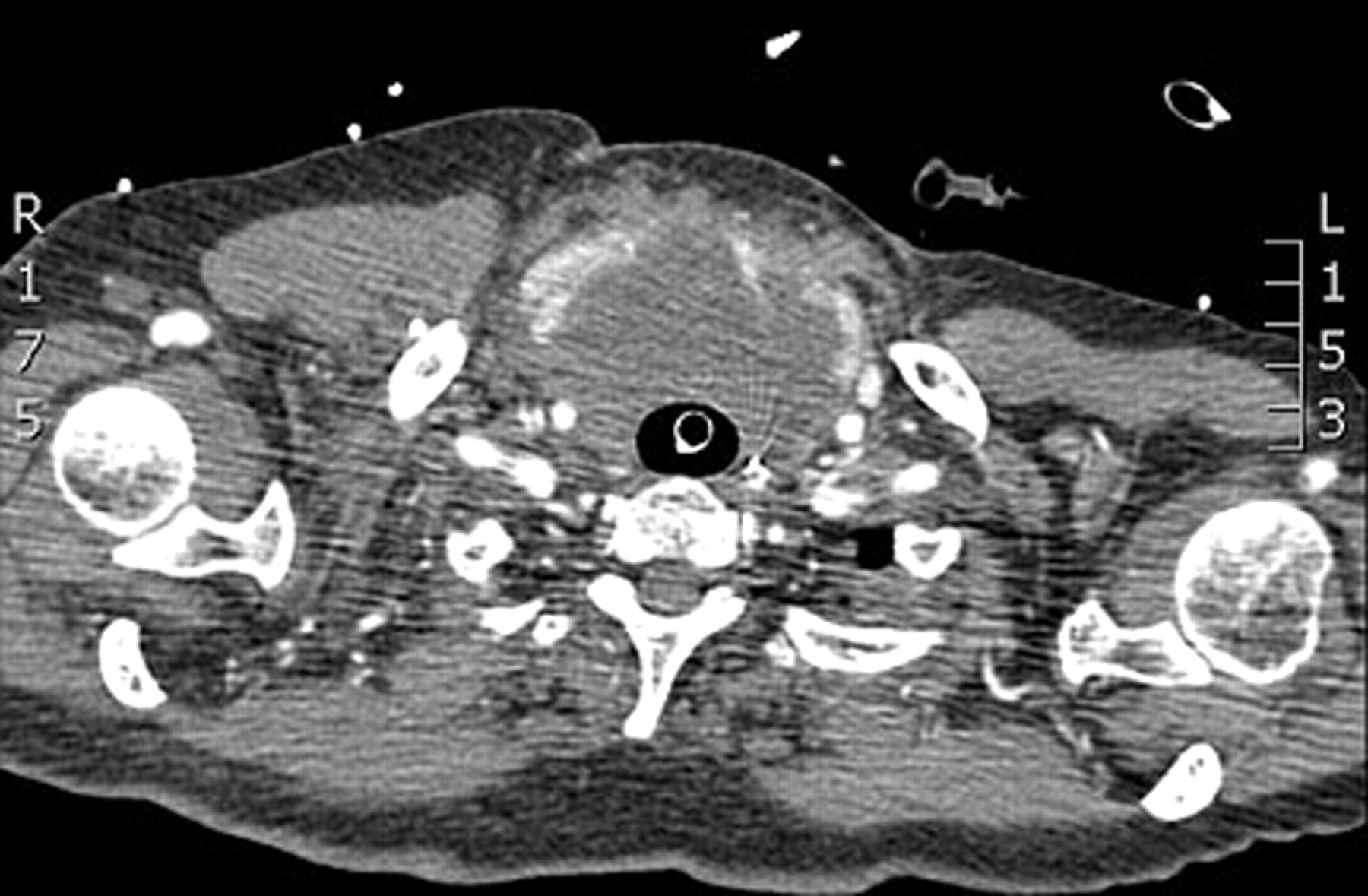
A CT scan of the thorax revealed no signs of pulmonary embolism. CT of the neck revealed diffuse enlargement of the thyroid gland (multinodular struma) with compression on the trachea. An inhomogeneous mass of the thyroid, measuring 7.5×6 cm, was seen (fig 1). Locoregional enlarged nodes were detected. Due to mass obstruction the tracheal diameter was reduced. The ET tube provided a patent airway, but more distally the trachea was almost completely compressed.

Macroscopy. Left-sided hemithyroidectomy mass.
Thyroid ultrasonography demonstrated multiple noduli with variable echodensity resembling multinodular struma with necrosis and possible haemorrhage (fig 2).

Preoperative CT image. Thyroid mass with tracheal compression.
An echocardiogram revealed good left and right ventricular function with normal atrial diameters and minor mitral and tricuspid regurgitation, excluding a cardiac origin of the collapse. CT of the cerebrum was normal.
TREATMENT
A left-sided hemithyroidectomy and a surgical tracheostomy (due to tracheomalacia) were performed suspecting a multinodular struma. Histology revealed a B cell lymphoma. An immunohistochemistry stain performed on bone marrow aspirate material demonstrated a population of lymphoid cells that were positive for CD20. Staging, including thoracoabdominal scanning and bone marrow biopsy showed no other tumour localisations.
Therapy with high dose prednisone and vincristine was initiated to reduce tumour size and to preserve the airway (resulting in rapid volume reduction and airway expansion).
OUTCOME
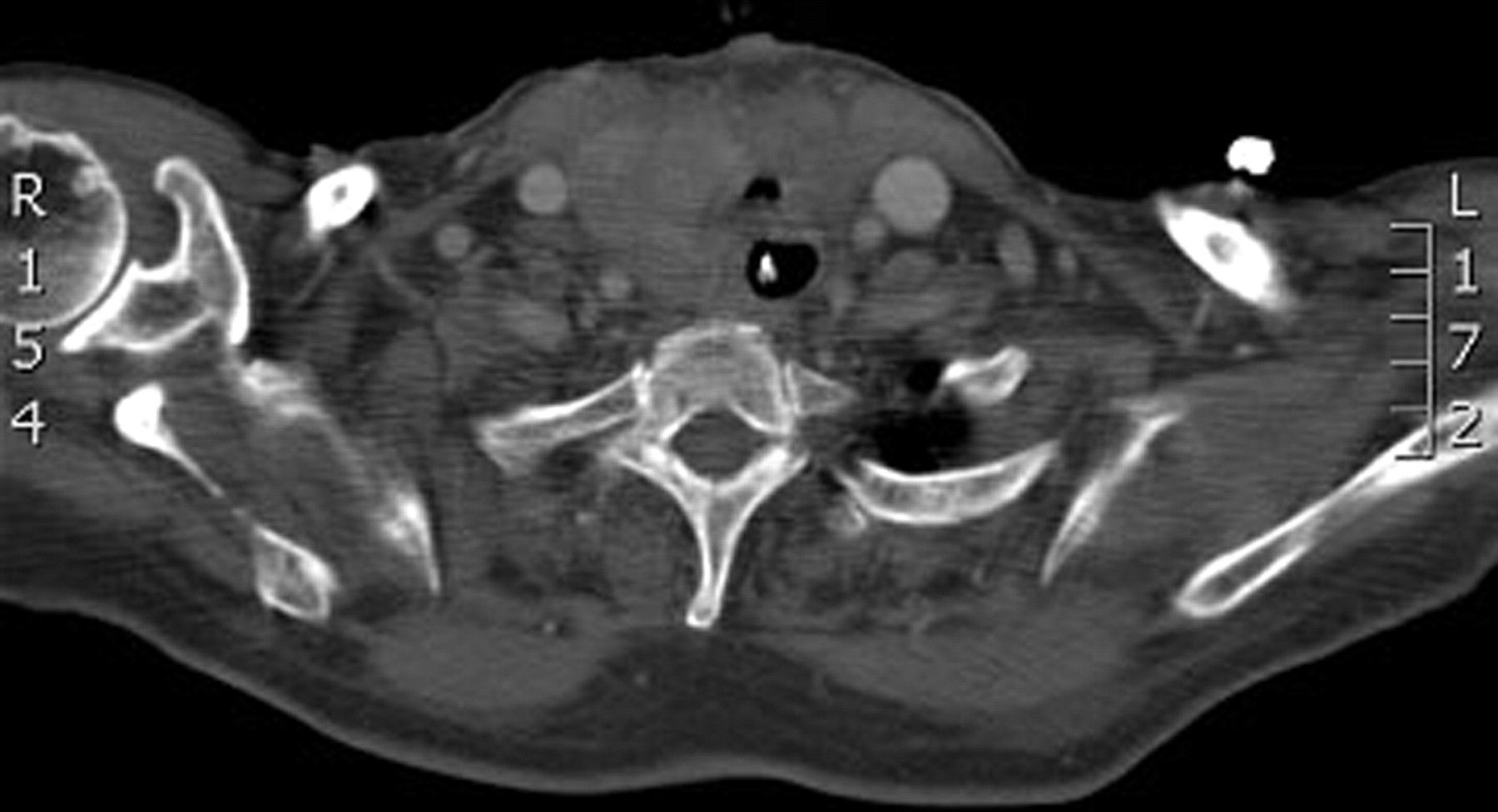
Within several days the patient could be weaned off of her tracheostoma tube due to a decrease in tumour mass. There were no signs of tumour lyses syndrome. She was discharged from the hospital after 4 weeks without further sequelae (fig 3).

Postoperative CT image. Post left-sided hemithyroidectomy. Tracheal compression resolved.
DISCUSSION
Upper airway obstruction in adults is most often due to aspiration of foreign bodies. Incomplete airway obstruction presents with stridor and respiratory distress or apnoea during sleep. In individuals with already anatomically narrow upper airways, the effects of sleep predispose them to inspiratory flow limitation (hypopnoeas), airway closure and obstructive sleep apnoea. Obstructive sleep apnoea syndrome is often a cause of obstruction in obesity. Incomplete obstruction can be further caused by allergic reactions (bee sting, peanuts, antibiotics), direct neck trauma, chemical burns and inhalation of toxic agents. Inflammation (tonsillitis and peritonsillar abscess), mass lesions of the pharynx, larynx or thyroid, neurological/neuromuscular diseases (vocal cord paralysis, Arnold–Chiari malformation) and tracheomalacia (due to long-term intubation) can also lead to airway obstruction. Laryngeal or pharyngeal carcinomas are causes of chronic obstruction often associated with prolonged smoking and alcohol ingestion. Upper airway obstruction can rapidly deteriorate leading to respiratory arrest and death. Therefore, the management in all causes of upper airway obstruction is to first secure the airway by placing an endotracheal tube or performing a tracheostomy. After that, imaging can be performed. A plain chest x ray can be performed to exclude vascular anomalies. CT scanning produces excellent resolution of images to evaluate the soft tissue and the osseous structures of the pharynx–larynx complex. To visualise laryngeal (including vocal cords) or pulmonary causes of airway obstruction, laryngoscopy or bronchoscopy is the investigation of choice.
Primary thyroid lymphoma is rare and represents 5% of all thyroid malignancies.1–4 It occurs in less than 1% of all non-Hodgkin’s lymphomas.2 It commonly occurs in older women with a history of Hashimoto thyroiditis/chronic thyroiditis, commonly presenting as a rapidly enlarging mass in the thyroid leading to hoarseness, dysphasia and dyspnoea.2–4
The vast majority of primary thyroid lymphomas are B cell in origin.4 Diffuse large B cell lymphoma and mucosa-associated lymphoid tissue (MALT) lymphoma are the most common subtypes. T cell lymphomas are extremely rare.4
The thyroid gland contains no native lymphoid tissue. Thus, migration of lymphoid tissue into the thyroid gland during an inflammatory or immunological process (eg, autoimmune thyroiditis/Hashimoto thyroiditis) can lead to thyroid lymphoma.1 Chronic antigenic stimulation of lymphocytes that takes place in autoimmune disorders may lead to a subpopulation of lymphocytes that are more susceptible to neoplastic transformation.4 As Hashimoto thyroiditis has a female predominance, primary thyroid lymphoma occurs more often in women.
The bicytopoenia, as described in our case, is likely due to the autoimmune mechanism in which the patient’s T lymphocytes suppress haemopoietic stem cells. This leads to autoimmune haemolytic anaemia and thrombocytopoenia. The inflammatory origin of the disease leads to leukocytosis (due to neutrophil increase) rather than leukocytopoenia. The bicarbonate level was markedly elevated, reflecting the subacute nature of the thyroid lymphoma.
The differential diagnoses for thyroid mass includes: abscess/infection, haemorrhage into a benign nodule, subacute or acute thyroiditis, anaplastic carcinoma, metastatic cancer, or thyroid lymphoma.1 Thyroid lymphoma should be kept in the differential diagnosis of goitre or thyroid nodules (see above). The diagnosis, however, remains difficult because there are no specific diagnostic tests to detect the occurrence of lymphoproliferative disorders. It is controversial whether reliable diagnosis of thyroid lymphoma is possible on the basis of a fine needle aspiration (FNA).4
T cell lymphomas are associated with a worse prognosis than B cell lymphomas.4
Due to the high proliferation rate of these tumours, they are very sensitive to cytotoxic chemotherapy. Rapidly progressive obstructive manifestations can lead to airway compromise. Therefore, therapy has to be initiated immediately once the diagnosis has been made.
The treatment of choice for thyroid lymphoma is medical and not surgical.
Frozen section pathology (fig 4) is often used for these rapidly enlarging thyroid masses (lymphoma or anaplastic carcinoma). If the pathologist finds one of these two tumours, it is better to end the operation because surgery for these two tumours has a higher risk for recurrent laryngeal nerve palsy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pathology slide. A. Low power magnification (2.5×) of the thyroid surrounded by partly necrotic lymphoid tissue. B. The higher magnification (40×) shows large atypical lymphoid cells, which were positive for CD20 (not shown).
The prognosis usually is favourable because this condition typically presents with localised disease, which is amenable to treatment with chemotherapy and radiation.
In conclusion, this case is an illustration of progressive respiratory distress due to airway compromise as a very unusual primary presentation of a thyroid lymphoma.
LEARNING POINTS
-
Thyroid lymphoma can present as an expanding thyroid mass with progressive respiratory distress.
-
The treatment of choice for thyroid lymphoma is medical and not surgical.
-
Rapid initiation chemotherapy results in rapid improvement.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.