Article Text

Summary
Takayasu’s arteritis is a systemic vasculitis predominantly affecting the aorta and its major branches. We report a 14-year-old girl in whom incidentally a deep upper limb vein thrombosis was found. She was referred to the emergency unit due to swelling and intermittent cyanosis of the right arm following an axillary depilatory wax. High-resolution echo colour Doppler ultrasonography showed a deep vein thrombosis with thickening of the proximal common carotids. A diagnosis of type IIb Takayasu’s arteritis was made. The patient’s history revealed fatigue, myalgia and headache. Immunosuppressive treatment and anticoagulation were introduced with a rapid and sustained improvement.
Statistics from Altmetric.com
BACKGROUND
We report a case of Takayasu’s arteritis, which presented with a misleading onset consisting of right upper limb swelling and intermittent cyanosis following an axillary depilatory wax. Provided that the early inflammatory periods of Takayasu’s arteritis includes non-specific symptoms and signs, general practitioners and paediatricians should consider Takayasu’s arteritis in the differential diagnosis, especially in the paediatric population. An early recognition and an aggressive treatment are crucial in reducing compromise of vital organs and mortality.
CASE PRESENTATION
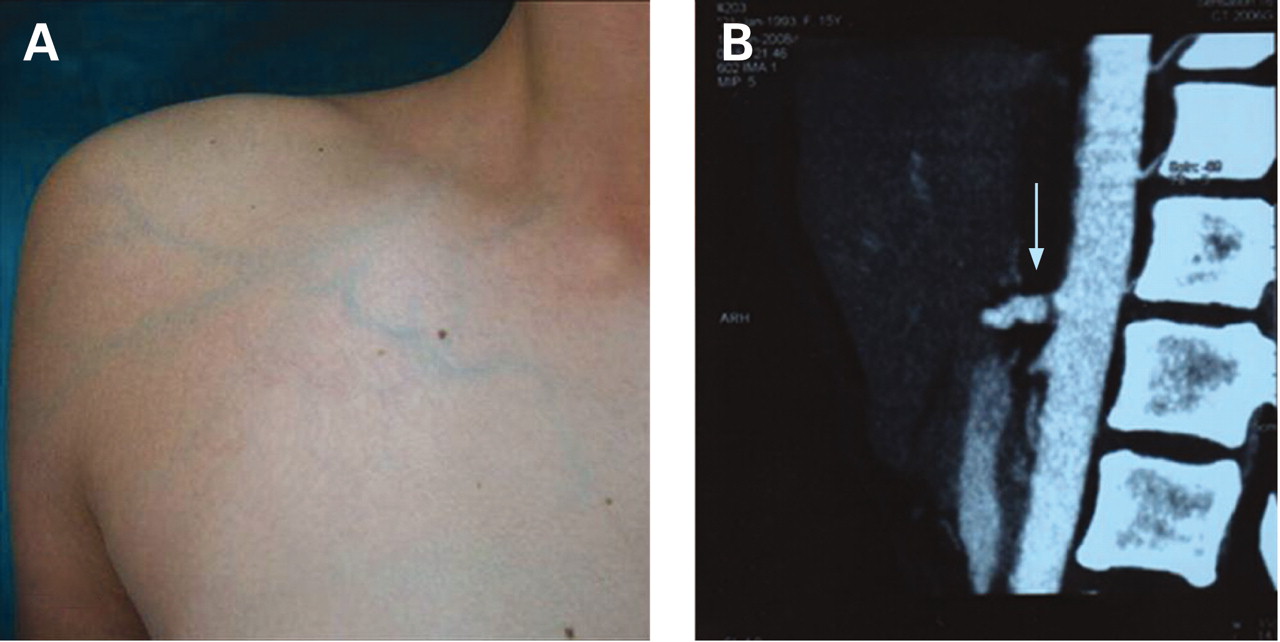
In June 2008, a 14-year-old Caucasian girl was referred to the emergency unit of our hospital for a swollen, painful and intermittently cyanotic right arm of sudden onset. The day before axillary depilatory wax was recorded. On physical examination she presented with lymph node enlargement on the right armpit without skin erythema. Right upper limb was cyanotic and cold when it was adducted while it was pink and warm on abduction. Venous network was evident in the subclavear, deltoid and brachial regions of the right arm (fig 1A). Family history and her past medical history were unremarkable. The girl was alert and afebrile; her heart rate was 80 bpm and the respiratory rate was 20/ min; brachial pulses as well as all others pulses were felt and symmetric. Nevertheless, a difference of systolic blood pressure between the two arms was detected with 110/70 mm/Hg on her left arm and 100/65 mmHg on the right arm. An infection was suspected and the provisional diagnosis was reactive lymphadenitis. Large spectrum antibiotic treatment was started (amoxicillin 1 g/day) without significant benefit.
{kind=link}
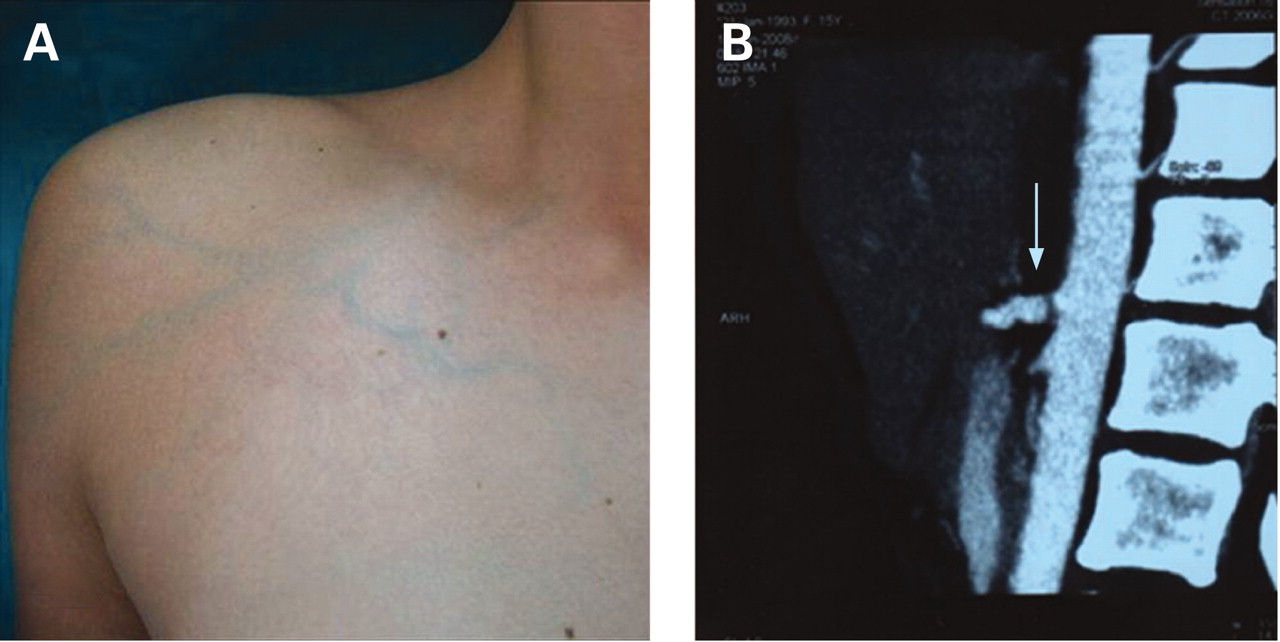
(A) Superficial venous network of the right arm. (B) MR angiogram shows irregularity and wall thickening of thoracic aorta and stenosis of celiac trunk (arrow).
INVESTIGATIONS
On admission, blood tests, including erythrocyte sedimentation rate (Westergren), C-reactive protein, full blood count, transaminases, serum creatinine, electrolytes and urinalysis were all normal. Electrocardiography, 2D echocardiogram and chest x ray were not contributory. Conversely, high-resolution echo colour Doppler (ECD) ultrasonography revealed a severe right axillary, omeral and subclavian vein thrombosis coupled with thickened wall of proximal common carotids. An exhaustive diagnostic work-up, including autoantibodies (anti-double-stranded DNA, anticardiolipin antibodies, lupus anticoagulant and anti- beta (2) glycoprotein I, antineutrofil cytoplasmic), was in the normal range. Screening for genetic and acquired thrombophilias (homocysteine, antithrombin, protein C, protein S, Factor V Leiden, activated protein C resistance) showed normal values. Tuberculin skin test was negative. Total body gadolinium-enhanced MR angiography confirmed the ultrasound findings and additionally revealed a celiac trunk and mesenteric artery stenosis with mild wall irregularity in the thoracic aorta (fig 1B). Cerebral and renal vessels were spared. Opthalmoangiopathia was excluded by fundoscopy.
At this point, her medical history was again investigated resulting helpful in the correct diagnosis. Indeed, by the age of 7 years the girl had suffered from leg numbness and pains, especially during physical activity and growing pains were diagnosed. At 13 years, she had a single episode of syncope with secondary seizures consisting of a brief period of unresponsiveness followed by sudden falling and tonic stiffening. Then, she experienced exercise intolerance climbing stairs and complained of myalgia and headache by 5 months prior to admission to the hospital. Thus, according to the American College of Rheumatology criteria, Takayasu’s arteritis was diagnosed.1 Consistent with the new angiographic classification of Takayasu’s arteritis based on the angiographic findings and vessel involvement, our case was defined type IIb.2 A full body F-18 fluorodeoxyglucose positron emission tomography (F-18 FDG-PET) scan revealed no active disease.3
OUTCOME AND FOLLOW-UP
Methylprednisolone pulses (30 mg/kg/day) for three consecutive days and, then, oral prednisone (2 mg/kg), immunosuppressive treatment (mycophenolate mofetil, 2 g/day) and oral anticoagulation (acenocoumarol 1.5 mg/day) were introduced with a rapid and sustained improvement of clinical symptoms. Surgical evaluation excluded revascularisation bypass surgery of abdominal aorta because of the absence of critical stenosis or occlusion. The girl was discharged on the day 16th from admission. She has been free of complications and there have been no cardiac events over the next months. At last visit, 7 months from diagnosis, ECD ultrasonography showed a partial recanalisation of right axillary and subclavian veins. Her last routine blood tests were all in the normal range; international normalised ratio was between 2 and 3 Units.
DISCUSSION
Takayasu’s arteritis is the third commonest chronic inflammatory granulomatous arteritis in childhood that mainly affects large vessels, predominantly the aorta, its main branches and pulmonary arteries.4,5 It leads to vessel wall thickening, fibrosis, stenosis and eventually thrombus formation. Different patterns of clinical, demographic and angiographic features of the disease have been described in various ethnic populations, with very few reports about childhood Takayasu’s arteritis.6–8
In our patient, the diagnosis was assessed according to the American College of Rheumatology Criteria for the Classification of Takayasu’s arteritis.1 The presence of three of the six following criteria is consistent with a diagnosis of Takayasu’s arteritis: onset age <40 years, claudication of an extremity, decreased brachial artery pulse, 10 mmHg difference in systolic blood pressure between the two arms, a bruit over the subclavian arteries or the aorta, and arteriographic evidence of narrowing or occlusion of the entire aorta, its primary branches or large arteries in the proximal upper and lower extremities. Furthermore, according to the new angiographic classification of Takayasu’s arteritis based on the angiographic findings and vessel involvement, the disease is now divided into six types: type I, the branches from the aortic arch; type IIa, the ascending aorta, aortic arch and its branches; type IIb, the ascending aorta, aortic arch and its branches, and the thoracic descending aorta; type III, the thoracic descending aorta, abdominal aorta and/or renal arteries; type IV, abdominal aorta and/or renal arteries; and type V, combined features of types IIb and IV).2 In our case, type IIb was the predominant pattern.
The anatomic-pathological findings reflect a classic triphasic pattern of Takayasu’s arteritis clinical symptoms and signs—namely, a systemic non-vascular phase, a vascular inflammatory phase and a quiescent “burnt out” phase.2,9 The diagnosis is extremely hard in the early inflammatory periods (phase 1 and 2), which are characterised by systemic complaints such as low-grade fever, arthralgia, myalgia, vertigo, breathlessness, weight loss, headache and arterial hypertension. At presentation, vascular symptoms are rare but become evident with the disease progression. Consequently, a delay between symptoms and diagnosis of 2 to 11 years is observed in juvenile as opposed to adult populations. Ischaemic findings (chest, limb and abdominal pain) and lack of peripheral pulses have been seldom reported in childhood.
As the active phase of Takayasu’s arteritis may be relatively short, and the disease can “burn out”, many cases remain undiagnosed. MR angiography may be particularly useful in detection of early signs of large-vessel disease and it has the added advantage of revealing evidence of ongoing vessel-wall inflammation.10 The disease activity can be also measured by CT and F-18 FDG-PET imaging in a non-invasive manner.11 Serological tests have proved unreliable in distinguishing active from quiescent disease.
The length of time between disease onset and institution of treatment is critical to the outcome because treatment is unlikely to alter vascular lesions in which fibrosis with narrowing has already taken place.12,13 It suggests that clinicians should consider the non-specific symptoms (low-grade fever, arthralgia, myalgia, vertigo, breathlessness, weight loss, headache) as important for a correct diagnosis. An early recognition of Takayasu’s arteritis is crucial to start an aggressive treatment with corticosteroids and immunosuppressants, which proved to be very successful. In our patient, the presence of an established collateral circle, a negative F-18 FDG-PET scan and negative MRI for acute vascular wall inflammation suggest that the disease had the acute phase years before in paediatrics age. The report shows the difficulty in diagnosing Takayasu’s arteritis in an earlier phase when the girl often complained of syncope and malaise. We hypothesise that the irritation caused by the application of depilatory wax was the trigger factor of thrombus enlargement leading to vascular compression that determined intermittent cyanosis.
This rare and underestimated condition should be encountered in the daily practice of both general practitioners and paediatricians in any young patient with non-specific symptoms leading to severe irreversible vessel damage if it remains disregarded.
LEARNING POINTS
-
A great delay between symptoms and diagnosis of Takayasu’s arteritis is observed in juveniles as opposed to adult populations; thus, a better awareness of Takayasu’s arteritis among paediatricians is required at present.
-
Non-specific constitutional symptoms, such as weakness, fatigue, weight loss and low-grade fever, were known to be the most common presenting features of Takayasu’s arteritis and were misdiagnosed. Ischaemic findings are seldom reported in childhood and pulses are often felt and are symmetric in the early phase of the disease.
-
As with all vasculitides, early diagnosis and prompt treatment are important in of Takayasu’s arteritis to prevent irreversible vessel damage with resulting compromise of vital organs.
Acknowledgments
We thank Professor Ignazio Pandolfo, Chief of Department of Radiological Sciences, Policlinico G. Martino Hospital, University of Messina, for his contribution to the patient’s diagnosis.
REFERENCES
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.