Article Text

Statistics from Altmetric.com
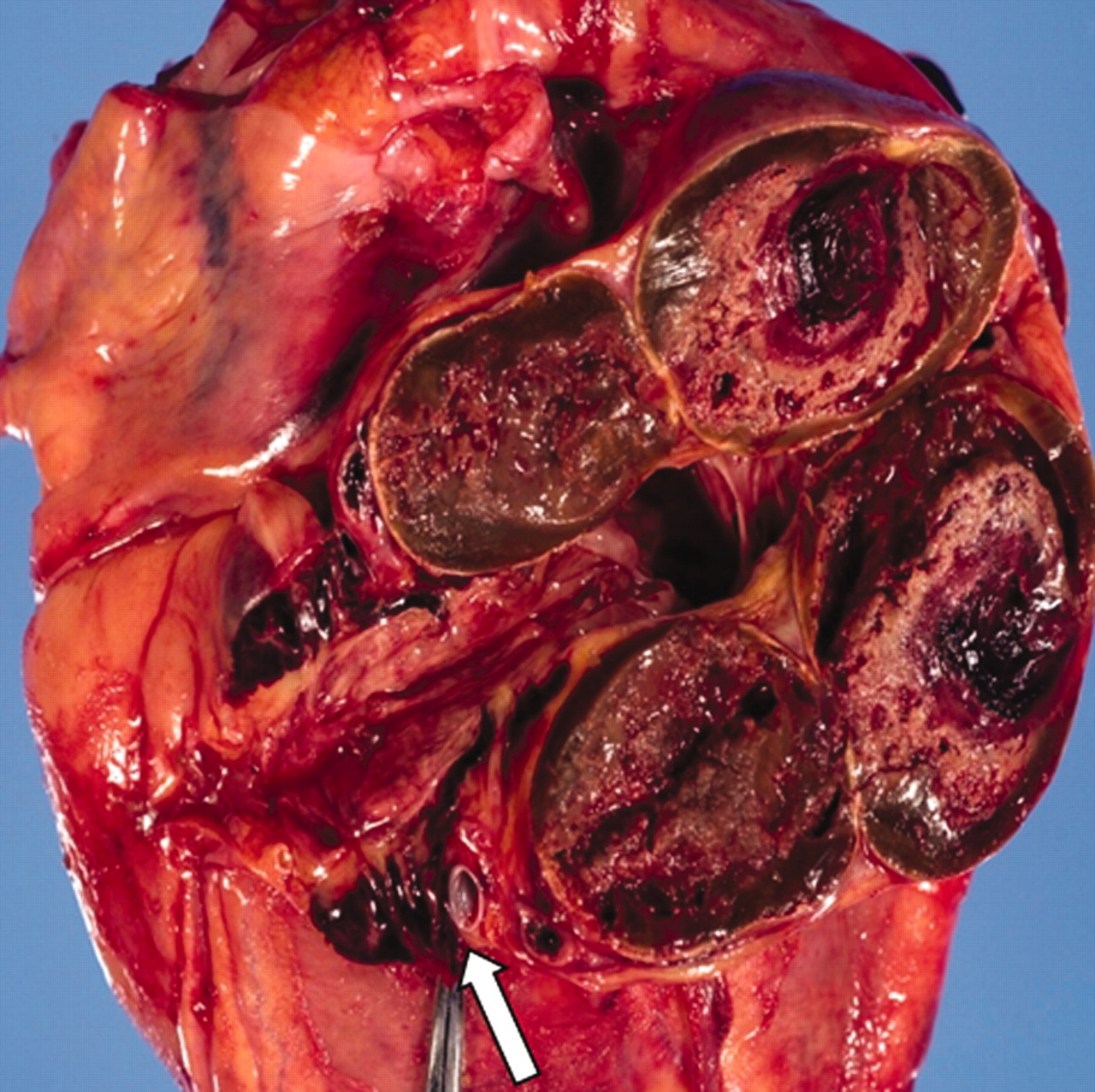
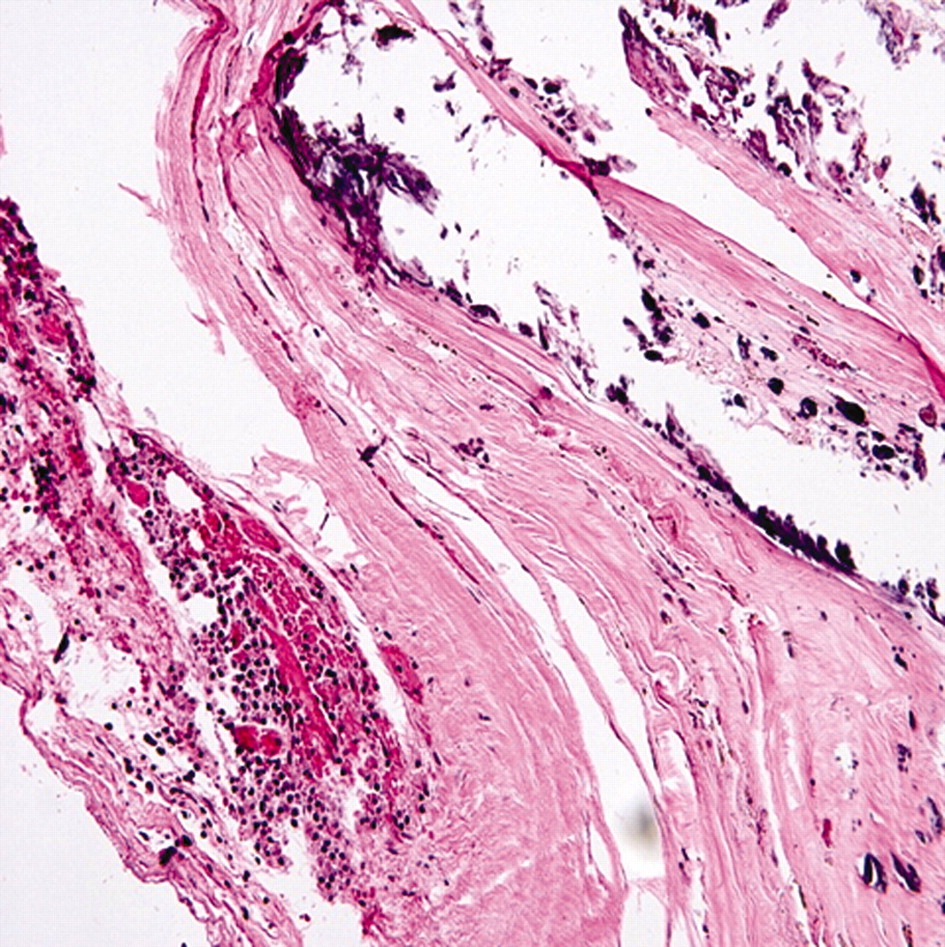
A 69-year-old hypertensive male smoker presented with acute inferior wall myocardial infarction. Cardiac catheterisation exposed an aneurysmal right coronary artery (RCA) with occluded lumen and an ectatic proximal left anterior descending artery (LAD). Chest computed tomography (fig 1) revealed a large calcified aneurysm with intraluminal thrombus. He underwent RCA bypass, but expired on the second day of surgery due to arterial suture dehiscence and haemorrhage. At autopsy the LAD had a proximal aneurysm (2.5 cm) and the RCA was found to have six discrete large saccular aneurysms (6, 2.2, 3, 6, 5 and 3.5 cm) (fig 2 shows two proximal aneurysms, arrow pointing to unaffected artery segment). RCA wall microscopy (fig 3) was suggestive of severe calcific atherosclerosis with few acute inflammatory cells related to surgery.



{kind=link}
{kind=link}
{kind=link}
By definition coronary artery aneurysms (CAAs) are aneurysmal dilatation >1.5 times the adjacent normal coronary segment. They are commonly related to an underlying atherosclerotic disease but higher prevalence has also been found in patients with Kawasaki’s disease, arteritis, mycoses, chest trauma, connective tissue disorders (Marfan’s and Ehlers–Danlos syndromes), metastatic tumours, polycystic kidney disease, percutaneous coronary interventions, idiopathic hypereosinophilic syndrome, coronary artery angiodysplasia and cocaine use.1–3 The reported incidence varies from 0.2–5.3%.3 Large CAAs of ⩾5 cm in adults unrelated to Kawasaki’s disease are extremely rare. Our case is the first report of such large saccular coronary aneurysms occurring at multiple sites along the vessel. Most patients with CAA are asymptomatic but may present with vasospasm, rupture, angina, myocardial infarction or stroke.3 Data on long term prognosis and optimal management is lacking yet most agree that coronary artery bypass surgery be performed in symptomatic patients.3
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication