Article Text

Statistics from Altmetric.com
Description
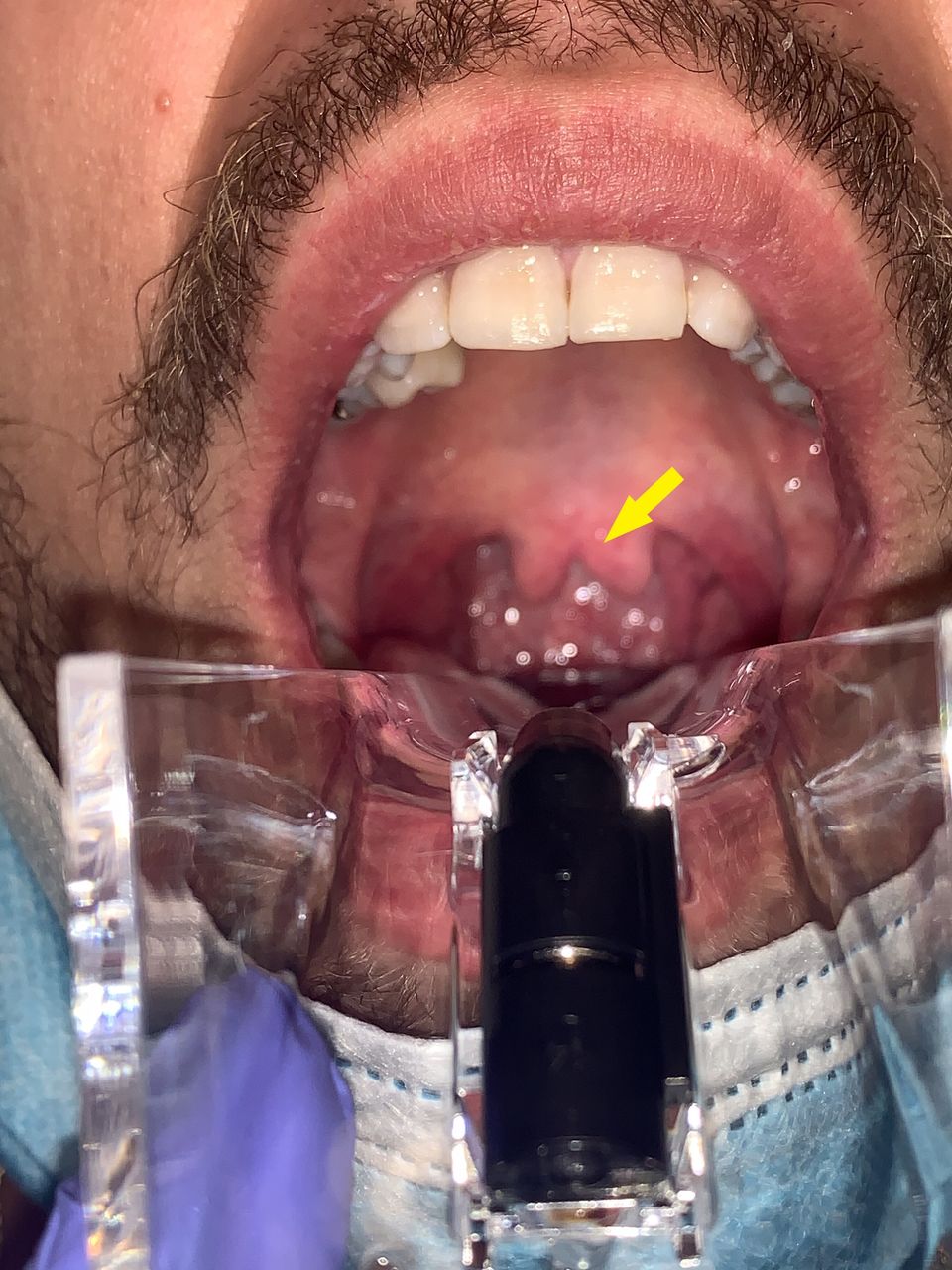
A 20-year-old man presented to the emergency department with a sore throat and general malaise for 2 days. On evaluation, an incidental bifurcated uvula was noted without any acute oropharyngeal abnormalities (figure 1). He reported the bifurcated uvula was likely congenital as his parents were informed of it shortly after his birth.

{kind=link}
Clinical photograph using a lighted speculum demonstrating a bifurcated uvula (arrow).
The patient denied any relevant medical history or any other known abnormalities since birth. A rapid group A streptococcus test was performed in the emergency department, which was negative. The patient was discharged with return precautions and primary care follow-up.
A bifid uvula or bifurcated uvula is a uvula with a visible cleft. While prevalence rates ranging from 0.18% to 10.3% have been documented throughout existing literature, with higher rates in South and East Asians and lower rates in Africans, the condition is often diagnosed and corrected in infancy and rarely found in adults.1–3 Though typically a benign finding with no consequence on airway integrity, a cleft uvula, along with nasal intonation, can indicate a submucosal cleft palate.4 Moreover, it has been shown to be sometimes associated with recurrent middle ear infections and nasal regurgitation during swallowing.5 However, our patient, although his voice may have been slightly nasal, did not have a notch in the back of the hard palate or translucency of the tissue along the middle of the soft palate, features that would suggest a submucosal cleft palate.
In rare circumstances, a bifid uvula can be associated with more serious complications. Patients with Loeys-Dietz syndrome (LDS), for which a bifid uvula is a common symptom, are at higher risk for aggressive arterial aneurysms, allergic and inflammatory disease, gastrointestinal inflammation and pregnancy-related complications for women with LDS.6 Our patient did not have any other typical LDS physical exam findings such as widely spaced eyes, strabismus or pectus excavatum. He denied history of aneurysms, joint laxity or the propensity to bruise easily.
Because the bifid uvula both is often benign and can also be associated with complications (most often speech abnormality due to nasal intonation and nasal regurgitation when swallowing), finding a bifid uvula in an adult patient is a rarity. Nevertheless, the possibility should not be overlooked in patients suspected for LDS or presenting with other associated signs and symptoms.
Patient’s perspective
Yeah, everyone always thinks it (my uvula) is so weird.
Learning points
A bifid uvula, while a rare but often benign sign, can sometimes be indicative of a submucosal cleft palate and is associated with recurrent middle ear infections and nasal regurgitation on swallowing.
Finding a bifid uvula in an adult patient is an extremely rare occurrence.
A bifid uvula, due to the potential association with Loeys-Dietz syndrome and the complications thereof, should not be dismissed when found despite its often benign tendency.
Ethics statements
Patient consent for publication
Acknowledgments
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare-affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Footnotes
Contributors MH saw the patient, documented patient’s course and took images. AG wrote description for accompanying images and edited submission. LG—submitting and corresponding author—edited description and compiled images, saw patient and obtained patient consent.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.