Article Text

Abstract
The artery of Percheron (AOP) is a rare arterial variant of the thalamic blood supply. Due to the densely packed collection of nuclei it supplies, an infarction of the AOP can be devastating. Here we highlight a patient who had an AOP stroke in the community, which was initially managed as cardiac arrest. AOP strokes most often present with vague symptoms such as reduced conscious level, cognitive changes and confusion without obvious focal neurology, and therefore are often missed at the initial clinical assessment. This case highlights the importance of recognising an AOP stroke as a cause of otherwise unexplained altered consciousness level and the use of MRI early in the diagnostic work-up.
- radiology (diagnostics)
- resuscitation
- stroke
- prehospital
- adult intensive care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
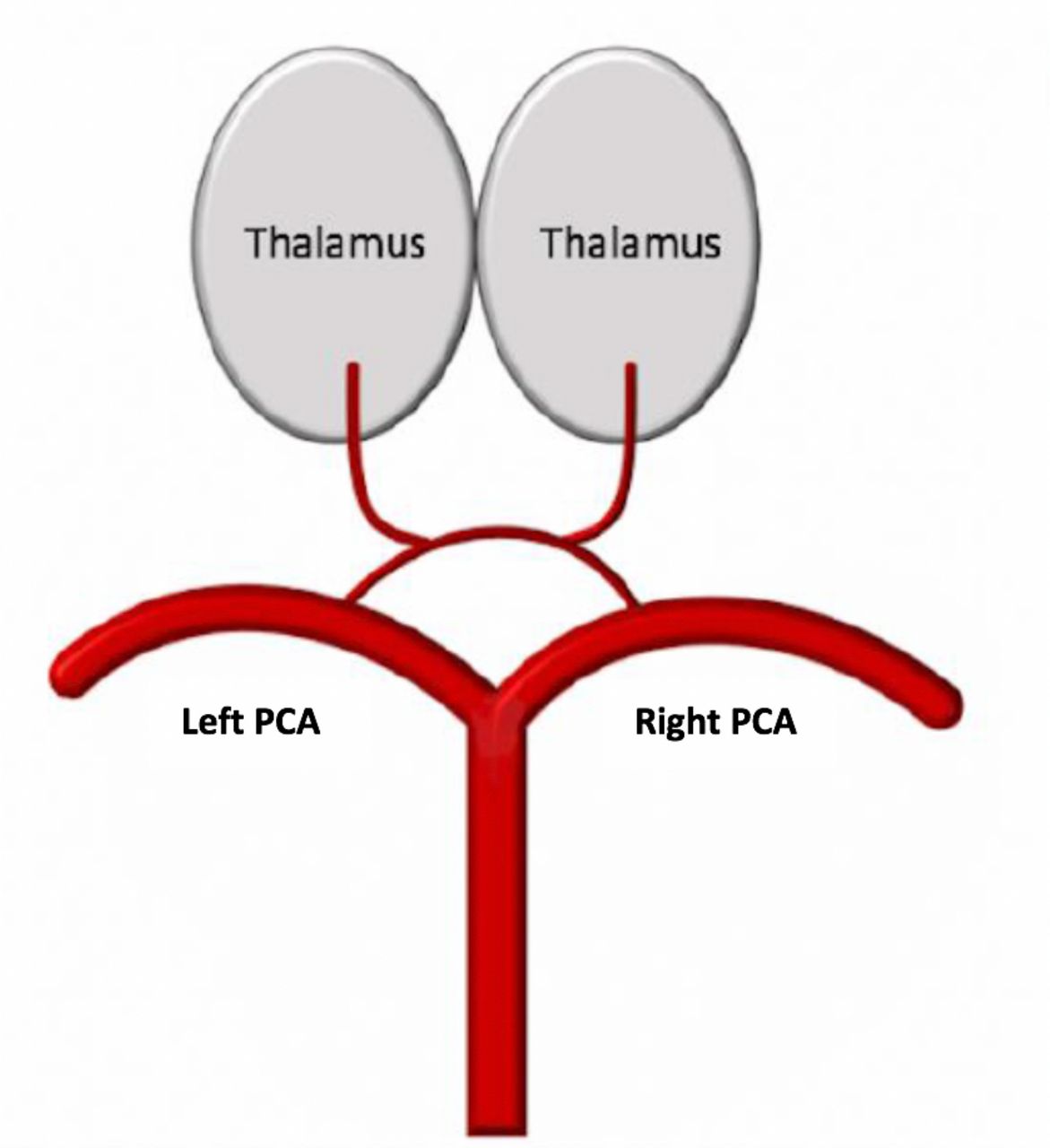
The artery of Percheron (AOP) is a rare anatomical variant of the paramedian branches of the posterior cerebral artery (PCA). The AOP is a single branch off the PCA that bifurcates to supply bilateral paramedian thalamic and bilateral rostral midbrain regions (figure 1).1 The most common triad of presentation of AOP infarcts is reduced consciousness, memory impairment and oculomotor disturbances.2–9 AOP infarcts are rare, but often result in permanent deficits and significant changes to patients’ functional abilities.10

Artery of Percheron anatomy; a single branch off the left or right PCA bifurcates to supply both thalami. Illustration by Dr Megan Quetsch. PCA, posterior cerebral artery.
Case presentation
A 79-year-old woman with a medical history of hypertension and mild Alzheimer’s dementia presented with acute onset loss of consciousness in the community. She was a passenger in a car and found to be unresponsive, with a family member reporting absence of a palpable pulse. She was presumed to have had a cardiac arrest and received 2 min of cardiopulmonary resuscitation in the community before the return of spontaneous circulation was noted. Paramedics arrived, and she was transported to a regional secondary hospital, triaged as a cardiac arrest. She was unresponsive with a Glasgow Coma Scale (GCS) of 3 and intubated on arrival. On arrival, she was in sinus rhythm with a heart rate of 84 beats/min. Her blood pressure was 140/110 mm Hg. The blood glucose reading was 6.7 mmol/L. Her neurological deficits were difficult to determine as she was unresponsive, but there was no obvious focal neurology. On examination, her lung fields were clear and she had dual heart sounds. There was no evidence of an infective aetiology on further history and examination. She was transferred to a tertiary hospital on the same day for further work-up in light of her ongoing reduced level of consciousness. The patient was extubated 24 hours later, with her GCS improving to 13–14 over the next day.
Investigations
CT of the brain and CT angiogram (CTA) were performed at the regional hospital 3 hours after the acute onset of symptoms. CT scan showed no evidence of ischaemic damage. CTA showed no filling defects, significant stenosis or aneurysmal changes. Blood tests, including complete blood examination, renal function, electrolytes, C reactive protein and creatine kinase were normal. Telemetry showed normal sinus rhythm. Electroencephalogram showed no evidence of seizure activity. MRI of the brain was requested the day after her symptom onset but not done urgently as there were no focal neurological findings. MRI of the brain was completed 72 hours after the onset of her symptoms and revealed symmetrical, bilateral thalamic diffusion restriction consistent with an AOP infarction (figure 2).

MRI demonstrating bilateral, symmetrical, thalamic diffusion restriction.
Later on, during her admission, an echocardiogram was performed and showed a concentric increase in left ventricular wall thickness suggestive of cardiac amyloidosis. On further haematological work-up, she had raised lambda light chains (442.50 mg/L (reference 5.71–26.3 mg/L)) and Bence-Jones proteinuria (456 mg/L (reference 0 mg/L)) suggestive of a plasma cell disorder. A bone marrow biopsy was not performed. Her skeletal survey was normal.
The patient’s family reported that the patient had lost 12 kg of weight in the past 12 months. She had CT scans of the chest, abdomen and pelvis prior to her current presentation through her general practitioner, and these did not show any significant pathology. Her weight loss was attributed to plasma cell disorder and further investigations were not pursued at this stage.
Outcome and follow-up
The patient’s GCS remained 13–14 throughout her admission, with persistent cognitive impairment and disorientation. She was found to have a vertical gaze palsy, which had not been noted earlier due to poor patient compliance with examination on admission. The patient was discharged to a stroke rehabilitation centre for ongoing therapy 11 days after her stroke, with a National Institutes of Health Stroke Scale score of 5 and a modified Rankin Scale score of 4. She was discharged from stroke rehabilitation to a residential care facility 5 weeks after her AOP infarction with residual cognitive deficits, mild global weakness, and expressive and receptive aphasia.
Discussion
The thalamus is a paramedian structure mainly composed of grey matter that controls a wide array of neurological functions including cognition, memory, sensation, motor functions, vision and arousal levels by acting as a relay centre.11 12 The thalamus consists of approximately 60 densely packed nuclei that transmit signals from nearly all efferent and afferent pathways, and therefore infarction in this region can present with a myriad of symptoms that can be easily missed on clinical evaluation.11
The thalamus is divided into four major vascular territories. These are the anterior, inferolateral, paramedian and posterior territories, determined by their arterial blood supply (figure 3).4 13–15 The anterior territory is supplied by the tuberothalamic artery, a branch of the posterior communicating artery. The inferolateral thalamic territory is supplied by the thalamogeniculate arteries which originate from the P2 segment of the PCA. The paramedian territory is generally supplied by the paramedian arteries, also known as the thalamic–subthalamic arteries, arising from the P1 segment of the PCA. The posterior choroidal arteries, stemming from the P2 segment of the PCA, supply the posterior thalamic territory.

Arterial supply of the thalamus, with associated four major vascular territories demonstrated. Adapted from Renard et al.15
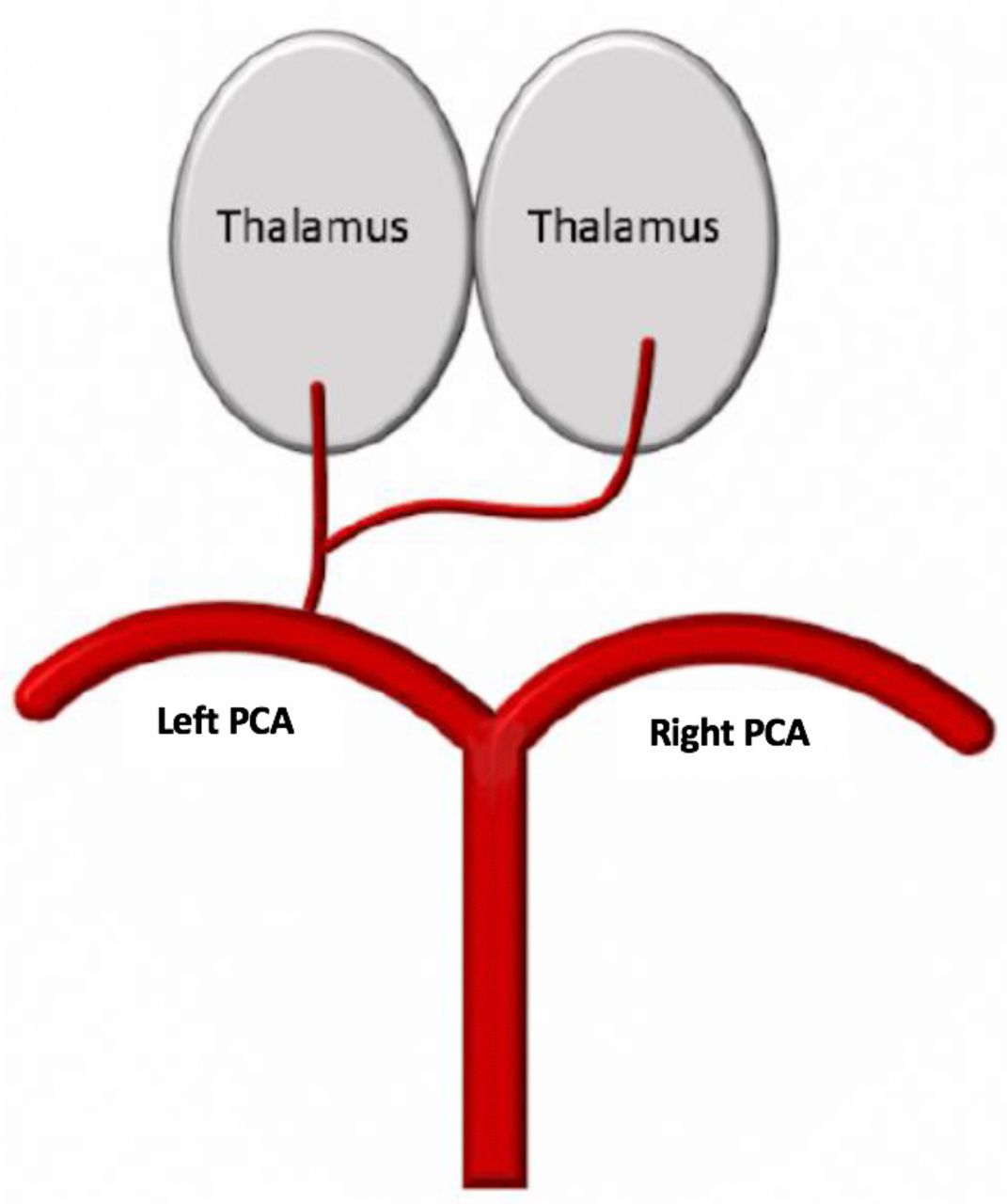
The exact number, location and structure of arteries supplying the thalamus can vary greatly. For example, the paramedian arteries often differ among individuals. Gerald Percheron first outlined the anatomical variations of the paramedian arteries in 1973. Percheron described four paramedian artery variants. Most commonly, the paramedian arteries arise separately from the right and left PCA to supply the respective right and left paramedian territories of the thalamus (figure 4). However, in a rare variant, known as the AOP, a single branch off the P1 segment bifurcates to supply bilateral paramedian thalamic territories and can also supply bilateral rostral midbrain territories (figure 1). Other more common variants of the paramedian arteries are illustrated in figures 5 and 6. In some individuals, the tuberothalamic artery is absent, and the AOP also supplies the anterior territory of the thalamus bilaterally.4 16 The prevalence of the AOP is not well studied, but in a small cadaveric study, the AOP was present in 11.7% of cases.17 Infarction of the AOP is a rare event, occurring in just 0.1%–2% of all strokes.1 As a single artery supplying bilateral thalamic territories, infarcts of the AOP present with significant deficits.

Normal anatomy of paramedian arteries. Paramedian arteries stem from both the right and left PCAs to supply respective paramedian thalami. Illustration by Dr Megan Quetsch. PCA, posterior cerebral artery.
Alternative paramedian artery anatomy. The paramedian arteries arise from an arterial branch traversing between the left and right P1 segments. Illustration by Dr Megan Quetsch. PCA, posterior cerebral artery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
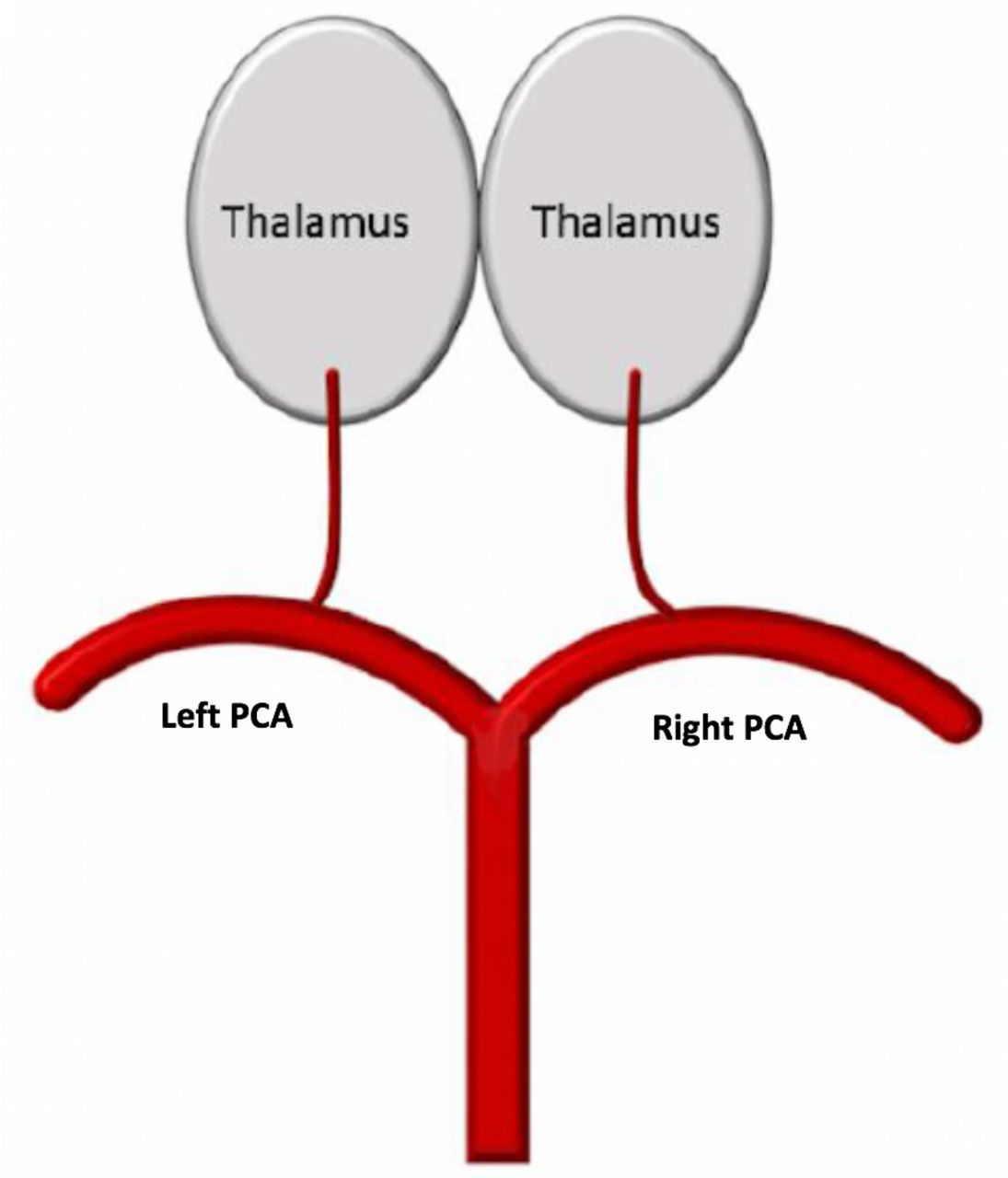
Alternative paramedian artery anatomy. Both paramedian arteries arise separately from the same P1 segment. Illustration by Dr Megan Quetsch. PCA, posterior cerebral artery.
An AOP infarction most often presents with reduced consciousness, cognitive impairment and vertical gaze palsy.4–9 12 18 There are few reported cases of AOP infarction in the literature presenting with sudden onset of coma requiring intensive care treatment. In all these cases, the initial CT scans were normal with subsequent MRI confirming bilateral thalamic infarcts as seen in our case.19 20 Additional symptoms may be present if there is involvement of the bilateral rostral midbrain and anterior thalamus. If the rostral midbrain is involved, patients may also present with ataxia or hemiparesis. 6 ,16 If the area of infarction involves the bilateral anterior thalamic territories, these patients generally present with more severe memory impairment.6 16 A 2010 retrospective study of 37 cases of AOP infarcts revealed that 43% of patients had bilateral paramedian thalamic infarcts with midbrain involvement, 38% of patients had bilateral paramedian thalamic infarcts without midbrain involvement, and 14% of patients had bilateral paramedian and anterior thalamic involvement as well as bilateral midbrain involvement.16
It is less likely that our patient actually had a cardiac arrest as reported by the family and the ambulance staff. Her subsequent ECGs were normal, and the serial troponins were found to be within normal limits. She did not undergo a coronary angiogram, but the echocardiogram showed possible evidence of cardiac amyloidosis with left ventricular thickening without any evidence of segmental hypokinesia. We do not believe that there is a correlation between cardiac amyloidosis and her clinical presentation, although there was a likelihood of paroxysmal atrial fibrillation causing a cardioembolic AOP infarction.21 22 It is more likely that a prolonged unresponsive episode due to AOP infarction may have been managed as cardiac arrest. To our knowledge, this is the first reported case of an AOP stroke masquerading as a cardiac arrest.
The ambiguity of the presentation and the rarity of an AOP infarct often lead to delayed diagnosis. A presentation of reduced GCS requires exclusion of a multitude of causes, including infection, seizure, encephalopathy, drug toxicity, cardiac causes and more. These cases are often not triaged as a stroke on arrival to the hospital and therefore do not receive urgent imaging required for diagnosis. AOP infarcts are rarely visualised on CT, which often further delays diagnosis and treatment.23 Most cases are diagnosed with MRI. As a result, reaching a firm diagnosis of an AOP infarction often occurs outside of the therapeutic window. There are few documented reports of AOP infarcts that were treated with intervention, with varied clinical outcomes reported post-treatment.7 24
This case highlights a rare and under-recognised stroke presentation. Although AOP occlusion accounts for only 0.1%–2% of all strokes, upto 4-35% of all thalamic infacrts could be due to AOP occulsion.1 ,3 It is important to consider a bilateral thalamic infarct due to AOP occlusion in patients who present with non-specific neurological findings, most notably with a triad of reduced consciousness, memory impairment and vertical gaze palsy.3–7 This case emphasises the importance of considering urgent MRI scanning in patients presenting with reduced GCS of unclear cause, as AOP strokes are rarely appreciated on CT. Greater recognition of the signs and symptoms of a bilateral thalamic infarct can result in earlier diagnosis of this debilitating stroke. With early recognition and urgent MRI scans, AOP strokes can be diagnosed within the therapeutic window, and these patients may have different outcomes.
Learning points
Artery of Percheron (AOP) strokes most often present with vague symptoms such as reduced conscious level, cognitive changes and gaze palsy, and therefore are often missed at the initial clinical assessment.
In a patient who presents with unexplained unresponsiveness, with normal CT and CT angiography, a stroke cannot be ruled out, and the patient should receive urgent MRI scanning.
If the cause of the unconsciousness or reduced level of consciousness is not clear after excluding the common causes, identifying an AOP stroke with the help of MRI scan within the therapeutic window for thrombolysis can be lifesaving as there are few cases of successful thrombolysis.
References
Footnotes
Contributors MQ and SN contributed equally. MQ wrote parts of the case presentation and discussion, and drafted the figures and images for the manuscript. MQ also consented the patient for publication. SN initiated the write-up. He also wrote several parts of the discussion, edited the manuscript several times and inserted a number of references. SH made some addition to the manuscript and did proofreading.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.