Article Text

Statistics from Altmetric.com
Description
An 80-year-old Caucasian man, presenting with polymyalgia and asthenia, was incidentally found to have a pancreatic mass. The patient underwent elective body-caudal pancreatectomy and splenectomy, with no major perioperative complications. Histopathological study revealed a 40-mm well-differentiated nonfuncting neuroendocrine tumour with peripancreatic adipose tissue extension, synaptophysin positive immunostaining, 5 mitoses/10 high power fields and a Ki67 proliferation index of 10% (G2, pT3N0, stage IIA). Postsurgery laboratory analysis and imaging studies (scintigraphy with [111In]In-pentetreotide) confirmed tumour remission.
Two years after the initial diagnosis, disease relapse was documented by a sudden rise in serum chromogranin A (588.1 ng/mL, n<85) and a positive [68Ga]Ga-DOTA-NOC ((1,4,7,10-tetraazacyclododecane-N,N’,N’’,N’’’-tetraacetic acid)-1-NaI3-octreotide) PET/CT scan that showed a 25 mm high uptake liver lesion in segment II with a maximum standardized uptake value (SUVmax:) of 80.5. Elective liver metastasectomy was performed and histological examination confirmed a secondary neuroendocrine lesion with a more aggressive Ki67 proliferation index (Ki67=15%, 7 mitoses/10 HPF). Subsequently, a decrease in chromogranin A was observed.
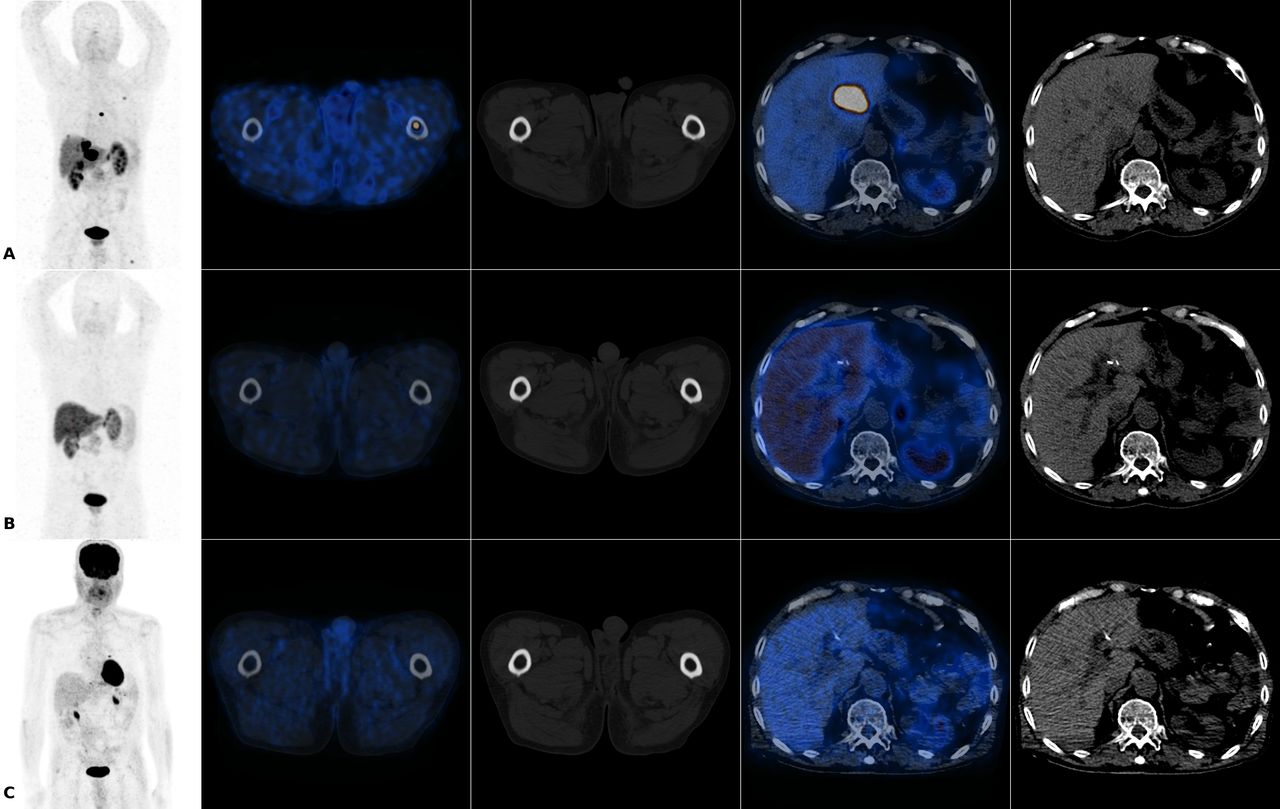
At the fourth-year postdiagnosis reevaluation, an increase in chromogranin A (394.2 ng/mL, n<85) was again noted. A restaging [68Ga]Ga-DOTA-NOC PET/CT scan (figure 1A) revealed four new hepatic lesions (segments II—SUVmax: 18.5, IV—SUVmax: 16.3, V— SUVmax: 6.2 and VII—SUVmax: 21.3) and bone metastases in the sternum (SUVmax: 1.8) and the second left costal arch (SUVmax: 1.3) with high somatostatin receptor expression. Additionally, a 2-[18F]FDG PET/CT scan showed increased glycolytic metabolism in three of the four known hepatic lesions (segments II—SUVmax: 5.4, V—SUVmax: 4.1 and VII—SUVmax: 7.6), suggesting a more aggressive disease. Thermoablation of the hepatic lesions was performed and lifelong lanreotide therapy started.
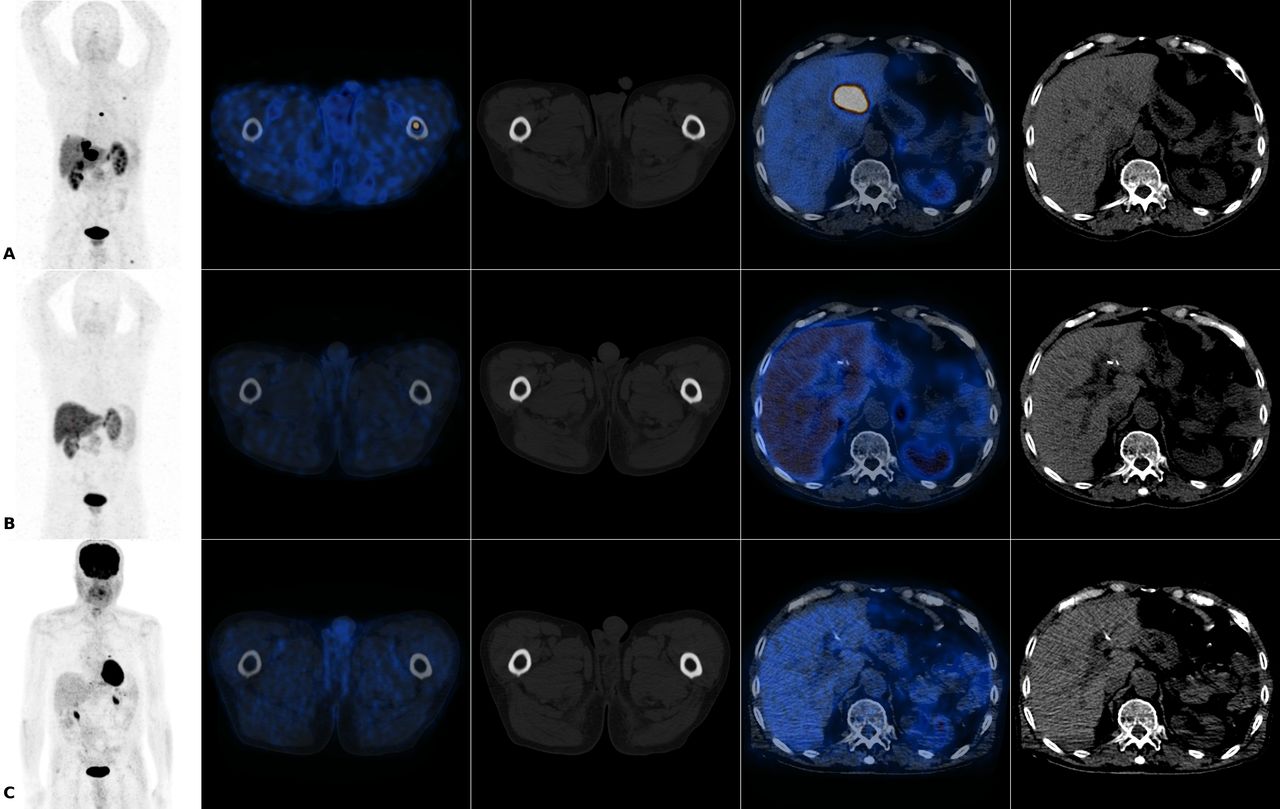
(A) January of 2017 [68Ga]Ga-DOTA-NOC PET/CT showing multiple hepatic and bone metastases with somatostatin receptors overexpression. (B, C) 2019 [68Ga]Ga-DOTA-NOC and 2-[18F]FDG PET/CTs, respectively, without evidence of differentiated or undifferentiated active disease. DOTA: 1,4,7,10-tetraazacyclododecane-N,N',N'',N'''-tetraacetic acid NOC: 1-Nal3-octreotide; PET: positron-emission tomography; 2-[18F]FDG: 2-[18F]fluoro-2-deoxy-D-glucose
Despite only presenting minor symptoms of abdominal discomfort and asthenia, chromogranin A serum levels kept rising, reaching a peak in February 2017 (1210 ng/mL, n<85), 5-year postdiagnosis. A [68Ga]Ga-DOTA-NOC PET/CT scan documented disease progression with new hepatic (segment III—SUVmax: 6.9) and bone lesions (proximal third of the left femoral diaphysis— SUVmax: 5.2), as well as significant increase in size and uptake of the previously known lesions (segments II—SUVmax: 108.0, IV— SUVmax: 40.1, V—SUVmax :8.9 and VII—SUVmax: 58.3, sternum, SUVmax: 13.1, second left costal arch—SUVmax: 4.7). The patient was deemed inoperable and proposed for peptide receptor radionuclide therapy (PRRT).
From March to October 2017, the patient underwent a total of four treatment cycles with [177Lu]Lu-DOTA-TATE (figure 2A-D), each with 7.4 GBq (cumulative activity of 29.6 GBq), using Aminoplasmal Hepa (2500 mL/cycle) for kidney protection. No haematological or renal toxicity was observed during therapy or follow-up. Clinical improvement in practically all quality of life indicators (as evaluated by EORTC QLQ-C30 questionnaire) was witnessed, particularly overall health status (17% in the first cycle and 50% in the fourth cycle), in addition to a 90% reduction in chromogranin A serum levels.

{kind=link}
{kind=link}
Twenty-four-hour posttherapy [177Lu]Lu-DOTA-TATE (luteium (1,4,7,10-tetraazacyclododecane-N,N’,N’’,N’’’-tetraacetic acid)-(Tyr3)-octreotate) scans. (A—D) Scan after first, second, third and fourth cycle of therapy, respectively.
Two years after PRRT, the patient maintains regular visits to the oncology department with no symptoms or evidence of active disease on both laboratorial and imaging studies, namely [68Ga]Ga-DOTA-NOC (figure 1B) and 2-[18F]FDG PET/CT (figure 1C).
Neuroendocrine neoplasms (NEN) are a very heterogeneous group of diseases, with increasing incidence and prevalence worldwide.1 These neoplasms can exhibit different receptors, and expression usually changes during the course of the disease.1–3 Screening tests are not readily available yet and patients often present with metastatic disease on initial evaluation.1
Multimodality imaging is strongly recommended and nuclear medicine techniques play a key role, namely [68Ga]Ga-DOTA-NOC and 2-[18F]FDG PET/CT. [68Ga]Ga-DOTA-NOC PET/CT evaluates somatostatin receptor expression, overexpressed in many of these neoplasms, and therefore has become indispensable for the diagnosis, staging and restaging, as well as PRRT patient selection. 2-[18F]FDG PET/CT assesses glycolytic metabolism, a crucial characteristic of aggressive molecular phenotypes, providing independent -prognostic information and also aiding in therapy selection.1 2 4
PRRT has become a new and useful option in the management of many NEN.1–9 Namely, outcome superiority over placebo or SSAs for midgut NEN has been established with high level evidence. Such is not the case, however, for pancreatic NEN, hindering its incorporation into international guidelines.3 5 Furthermore, many other radiation free therapies for pancreatic NEN are available and have been approved.5
That being said, pancreatic NEN have shown significantly higher response rates to PRRT when compared with other NEN.6 Some metastatic or inoperable pancreatic NEN patients are still alive more than 12 years after the beginning of PRRT.8 Additionally, some studies imply that repeated [177Lu]Lu-DOTATATE treatment cycles, in a so called salvage therapy setting, are feasible, with low incidence of myelodysplastic syndromes and no III/IV grade renal toxicity, and potential overall survival benefit.7 On functioning pancreatic NEN, PRRT has been shown to effectively control refractory carcinoid-syndrome symptoms, a very important cause for quality of life reduction.9 Nevertheless, in most cases, only a cytostatic effect is observed, increasing progression-free survival. Rarely, tumour burden reduction can be detected, but complete remission is seldom witnessed.3
As highlighted in this case, PRRT is an effective therapeutic option with a high safety profile in inoperable metastatic pancreatic NEN that, in some cases, even in aggressive molecular phenotypes, can induce complete remission. In addition, it underscores the importance of a multimodality approach in the management of NEN.
Patient’s perspective
I now rarely have pain and feel like a child that can do everything. I wake up every morning and go outside; it seems that I never get tired. Everyone in the Nuclear Medicine Department was very kind to me and I’d like to pay them a visit, even if further treatments aren’t needed.
Learning points
Gallium-68-labeled somatostatin analogues ([68Ga]Ga-DOTA-NOC) and fluor 18 - labeled glucose analogue(2-[18F]FDG) positron-emission tomography/computed tomography (PET/CT) play a key role in the diagnosis, staging and restaging of neuroendocrine tumours.
Peptide receptor radionuclide therapy is a safe and effective therapeutic option for the control of inoperable neuroendocrine tumours, with potential quality of life improvement.
Complete remission with lutetium-177 -labeled somatostatin analogues ([177Lu]Lu-DOTA-TATE), although rare, is possible in some cases.
Footnotes
Contributors PS and HM: conception and design, acquisition of data, analysis and interpretation of data, drafting the article. RS and APM: revising it critically for important intellectual content and the final approval of the version published. PS, HM, RS and APM: agreement to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.